
Table of Contents
As confidentially submitted to the Securities and Exchange Commission on February 13, 2018
Registration No. 333-
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM S-1
REGISTRATION STATEMENT
UNDER
THE SECURITIES ACT OF 1933
Electrocore, LLC*
(Exact name of Registrant as specified in its charter)
| Delaware | 3845 | 20-345-4976 | ||
| (State or other jurisdiction of incorporation or organization) |
(Primary Standard Industrial Classification Code Number) 150 Allen Road, Suite 201 Basking Ridge, New Jersey 07920 (973) 290-0097 |
(I.R.S. Employer Identification Number) | ||
| (Address, including zip code, and telephone number, including area code, of Registrant’s principal executive offices) | ||||
Francis R. Amato
Chief Executive Officer
Electrocore, LLC
150 Allen Road, Suite 201
Basking Ridge, New Jersey 07920
(973) 290-0097
(Name, address, including zip code, and telephone number, including area code, of agent for service)
with copies to:
| John L. Cleary, II, Esq. Ira L. Kotel, Esq. Dentons US LLP 1221 Avenue of the Americas New York, New York 10020 (212) 768-5359 |
Peter N. Handrinos, Esq. Nathan Ajiashvili, Esq. Latham & Watkins LLP 200 Clarendon Street Boston, Massachusetts 02116 (617) 948-6000 |
Approximate date of commencement of proposed sale to the public: As soon as practicable after the effective date of this Registration Statement.
If any of the securities being registered on this Form are to be offered on a delayed or continuous basis pursuant to Rule 415 under the Securities Act of 1933 check the following box: ☐
If this Form is filed to register additional securities for an offering pursuant to Rule 462(b) under the Securities Act, please check the following box and list the Securities Act registration statement number of the earlier effective registration statement for the same offering. ☐
If this Form is a post-effective amendment filed pursuant to Rule 462(c) under the Securities Act, check the following box and list the Securities Act registration statement number of the earlier effective registration statement for the same offering. ☐
If this Form is a post-effective amendment filed pursuant to Rule 462(d) under the Securities Act, check the following box and list the Securities Act registration statement number of the earlier effective registration statement for the same offering. ☐
Indicate by check mark whether the Registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, a smaller reporting company or an emerging growth company. See the definitions of “large accelerated filer,” “accelerated filer,” “smaller reporting company” and “emerging growth company” in Rule 12b-2 of the Exchange Act.:
| Large accelerated filer | ☐ | Accelerated filer | ☐ | |||
| Non-accelerated filer | ☒ (do not check if a smaller reporting company) | Smaller reporting company | ☐ | |||
| Emerging growth company | ☒ |
CALCULATION OF REGISTRATION FEE
|
| ||||
| Title of Each Class of Securities to be Registered |
Proposed Maximum Aggregate Offering Price(1)(2) |
Amount of Registration Fee | ||
| Common Stock, par value $0.001 per share |
$ | $ | ||
|
| ||||
|
| ||||
| (1) | Estimated solely for the purpose of calculating the registration fee pursuant to Rule 457(o) under the Securities Act. |
| (2) | Includes the estimated aggregate offering price of the shares issuable upon exercise of the underwriters’ option to purchase additional shares from us. See “Underwriting.” |
| * | Prior to the closing of the offering to which this Registration Statement relates, a corporate conversion will be effected such that the issuer of the common stock to be registered pursuant to this Registration Statement will be a Delaware corporation named electroCore, Inc. |
The Registrant hereby amends this Registration Statement on such date or dates as may be necessary to delay its effective date until the Registrant shall file a further amendment which specifically states that this Registration Statement shall thereafter become effective in accordance with Section 8(a) of the Securities Act of 1933 or until the Registration Statement shall become effective on such date as the Commission, acting pursuant to said Section 8(a), may determine.
Table of Contents
EXPLANATORY NOTE
Electrocore, LLC, the registrant whose name appears on the cover of this registration statement, is a Delaware limited liability company. Prior to the closing of this offering, Electrocore, LLC intends to convert into a Delaware corporation pursuant to a statutory conversion and change its name to electroCore, Inc. As a result of the corporate conversion, the holders of units of Electrocore, LLC will become holders of common stock and options to purchase common stock of electroCore, Inc. Holders of warrants to purchase units of Electrocore, LLC will become holders of warrants to purchase common stock of electroCore, Inc. See “Corporate Conversion.” Except as disclosed in the accompanying prospectus, the consolidated financial statements and selected historical consolidated financial data and other financial information included in this registration statement are those of Electrocore, LLC and do not give effect to the corporate conversion.
Table of Contents
The information in this preliminary prospectus is not complete and may be changed. We may not sell these securities until the registration statement filed with the Securities and Exchange Commission is effective. This preliminary prospectus is not an offer to sell these securities and it is not soliciting offers to buy these securities in any state where the offer or sale is not permitted.
Subject to Completion, Dated , 2018
Shares
ELECTROCORE, INC.
Common Stock

| • electroCore, Inc. is offering shares of its common stock.
• The initial public offering price of our common stock is expected to be between $ and $ per share. |
• This is our initial public offering and no public market currently exists for our common stock.
• We intend to apply for the listing of our common stock on The Nasdaq Global Select Market under the symbol “ECOR.” |
Investing in our common stock involves risks. See “Risk Factors” beginning on page 13 to read about factors you should consider before buying shares of our common stock.
We are an ‘‘emerging growth company’’ as defined under the U.S. federal securities laws and, as such, intend to comply with certain reduced public company reporting requirements for this and future filings.
| Per Share | Total | |||||
| Initial public offering price |
$ | $ | ||||
| Underwriting discounts and commissions(1) |
$ | $ | ||||
| Proceeds, before expenses, to electroCore, Inc. |
$ | $ | ||||
| (1) | We have agreed to reimburse the underwriters for certain expenses. We refer you to “Underwriting” for additional disclosure regarding total underwriting compensation. |
The underwriters have an option to purchase a maximum of additional shares to cover over-allotments.
Neither the Securities and Exchange Commission nor any state securities commission has approved or disapproved of these securities or determined if this prospectus is truthful or complete. Any representation to the contrary is a criminal offense.
Delivery of the shares of common stock will be made on or about , 2018.
| Piper Jaffray |
Evercore ISI | |
|
JMP Securities | ||
The date of this prospectus is , 2018
Table of Contents
| Page | ||||
| 1 | ||||
| 13 | ||||
| 63 | ||||
| 64 | ||||
| 65 | ||||
| 66 | ||||
| 68 | ||||
| 70 | ||||
| 72 | ||||
| Management’s Discussion and Analysis of Financial Condition and Results of Operations |
74 | |||
| 89 | ||||
| 143 | ||||
| 152 | ||||
| 164 | ||||
| 170 | ||||
| 173 | ||||
| 179 | ||||
| 181 | ||||
| 185 | ||||
| 192 | ||||
| 192 | ||||
| 192 | ||||
| F-1 | ||||
Neither we nor the underwriters have authorized anyone to provide you with any information other than that contained in this prospectus, any amendment or supplement to this prospectus or in any free writing prospectus we may authorize to be delivered or made available to you. The underwriters and we take no responsibility for, and can provide no assurance as to the reliability of, any other information that others
i
Table of Contents
may give you. We and the underwriters are offering to sell, and seeking offers to buy, shares of our common stock only in jurisdictions where offers and sales are permitted. The information contained in this prospectus is current only as of the date on the front of this prospectus, regardless of the time of delivery of this prospectus or any sale of shares of our common stock. Our business, financial condition, results of operations and prospects may have changed since that date.
For investors outside the United States: We have not, and the underwriters have not, done anything that would permit this offering or possession or distribution of this prospectus in any jurisdiction where action for that purpose is required, other than in the United States. Persons outside the United States who come into possession of this prospectus must inform themselves about, and observe any restrictions relating to, the offering of the shares of common stock and the distribution of this prospectus outside the United States.
MARKET DATA AND FORECASTS
Unless otherwise indicated, information in this prospectus concerning economic conditions, our industry, and our markets, including our general expectations and competitive position, market opportunity and market size, is based on a variety of sources, including information from independent industry analysts and publications, as well as our own estimates and research.
Our estimates are derived from industry and general publications, studies and surveys conducted by third-parties, as well as data from our own internal research. These publications, studies and surveys generally indicate that their information has been obtained from sources believed to be reliable, although they do not guarantee the accuracy or completeness of such information, and we have not independently verified industry data from such third-party sources. While we believe our internal research is reliable and that our internal estimates are reasonable, such research has not been verified by any independent source and our internal estimates are based on our good faith beliefs as of the respective dates of such estimates. We are responsible for all of the disclosure in this prospectus.
FINANCIAL STATEMENT PRESENTATION
The financial statements for the year ended December 31, 2016 represent the operations of Electrocore, LLC and its subsidiaries and affiliate. Prior to the closing of this offering, we will complete a corporate conversion pursuant to which electroCore, Inc. will succeed to the business of Electrocore, LLC and its consolidated subsidiaries and affiliate, and the unitholders of Electrocore, LLC will become stockholders and option holders of electroCore, Inc., as described under the heading “Corporate Conversion.” In this prospectus, we refer to this transaction as the “corporate conversion.” We expect that our conversion from a Delaware limited liability company to a Delaware corporation will not have a material effect on our consolidated financial statements at the time of the corporate conversion.
Pursuant to the applicable provisions of the Fixing America’s Surface Transportation Act, we are not required to file our financial information for the historical 2015 annual period and the nine month periods ended September 30, 2016 and 2017 because we expect to file our financial information for the year ended December 31, 2017 in the first public filing of our registration statement. While the 2015 and interim 2016 and 2017 financial information is otherwise required by Regulation S-X, we believe that it will not be required to be included in our registration statement at the time of the first public filing.
ii
Table of Contents
TRADEMARKS AND TRADENAMES
This prospectus includes our trademarks such as electroCore®, gammaCore® and gammaCore Sapphire™ which are protected under applicable intellectual property laws and are the property, prior to the corporate conversion discussed herein, of Electrocore, LLC, and after the corporate conversion, of electroCore, Inc. Solely for convenience, trademarks, service marks and tradenames referred to in this prospectus may appear without the ®, TM or SM symbols, but such references are not intended to indicate, in any way, that we will not assert, to the fullest extent under applicable law, our rights or the right of the applicable licensor to these trademarks, service marks and tradenames. This prospectus may also contain trademarks, service marks, tradenames and copyrights of other companies, which are the property of their respective owners.
GLOSSARY
A glossary of scientific and technical terms used throughout this prospectus is included beginning on page 140.
ABOUT THIS PROSPECTUS
Except where the context otherwise requires or where otherwise indicated, the terms “electroCore,” “we,” “us,” “our,” “our company,” and “our business” refer, prior to the corporate conversion discussed herein, to Electrocore, LLC, and after the corporate conversion, to electroCore, Inc.
iii
Table of Contents
This summary highlights certain information about us and this offering contained elsewhere in this prospectus. Because it is only a summary, it does not contain all the information that you should consider before investing in shares of our common stock and it is qualified in its entirety by, and should be read in conjunction with, the more detailed information appearing elsewhere in this prospectus. Before you decide to invest in our common stock, you should read the entire prospectus carefully, including “Risk Factors” beginning on page 13 and our consolidated financial statements and the accompanying notes included in this prospectus.
Overview
We are a commercial-stage bioelectronic medicine company with a platform non-invasive vagus nerve stimulation therapy initially focused on neurology and rheumatology. Our therapy, gammaCore, has pharmacologic effects on the peripheral and central nervous systems, which modulate neurotransmitters and immune function. gammaCore is FDA-cleared for the acute treatment of pain associated with migraine and episodic cluster headache in adults. In order to generate advocacy among physicians and patient demand in the form of prescriptions submitted to payors, we recently initiated a product registry for episodic cluster headache. Having established a base of advocacy among key opinion leaders in the headache field through the product registry, our strategy is to commercially launch in migraine and episodic cluster headache in the second quarter of 2018. Based on our clinical data, we are pursuing label expansions for the prevention of migraine, migraine in adolescents and post-traumatic headache, and are also engaging in clinical development for potential new labeling claims in rheumatology, including Sjôgren’s syndrome and rheumatoid arthritis.
gammaCore is the first FDA-cleared, prescription-only vagus nerve stimulation, or VNS, therapy administered in discrete doses using a proprietary, simple-to-use handheld delivery system. Our therapy activates the therapeutically relevant fibers in the vagus nerve. This is enabled by our proprietary high-frequency burst waveform that safely and comfortably passes through the skin and stimulates the targeted nerve fibers. The modulation of neurotransmitters by our therapy has a similar pharmacological effect to that of multiple classes of medications, including selective serotonin reuptake inhibitors, serotonin norepinephrine reuptake inhibitors, GABA analogues, acetylcholine esterase inhibitors and triptan medications, all of which are commonly prescribed. Research indicates that VNS therapy also modulates the immune system to produce anti-inflammatory effects comparable to therapies that inhibit inflammatory cytokines.
Background of Vagus Nerve Stimulation
The vagus nerve is the largest and most extensive cranial nerve, connecting the brainstem to nearly every organ in the chest and abdomen, including the heart, lungs, liver, stomach, spleen, kidneys, and digestive tract. Over the past two decades, the body of scientific evidence in support of VNS in multiple medical conditions has been growing. However, this potential has remained unfulfilled because the therapy could only be delivered using electrodes affixed to the vagus nerve, connected to a signal generator implanted in the chest wall. To implant these devices, the vagus nerve must be surgically exposed from its anatomical position entwined with the carotid artery.
Our Therapy Delivery Platform
gammaCore stimulates the vagus nerve through a simple-to-use handheld delivery system dispensing therapy on a 31-day prescription basis and, like medications delivered by metered-dose inhalers, patients self-administer discrete doses. Our delivery platform enables access to VNS for a much broader patient
1
Table of Contents
population than previously possible, making it a potential preferred treatment option. gammaCore’s successor, gammaCore Sapphire, is a rechargeable and reloadable version of our product intended for multi-year use. It is activated on a monthly basis through the input of a unique, prescription-only authorization code, delivered via a radio-frequency identification, or RFID, card. In the future, this authorization code may be delivered through the internet, leveraging the Bluetooth capabilities of gammaCore Sapphire.
Competitive Strengths
We believe the competitive strengths of our company and our novel and proprietary self-administered bioelectronic therapy include:
| • | Innovative bioelectronic medicine approach. Our gammaCore therapy uses a proprietary electric signal to safely deliver bioelectronic medicine, which causes targeted pharmacologic-like changes in neurotransmitter expression and in the immune system without systemic exposure to exogenous chemicals. |
| • | Our non-invasive therapy unlocks the long-held potential of VNS. VNS therapy can, for the first time, be delivered comfortably through the skin using gammaCore. This eliminates the need for costly, invasive surgery that has been reserved for the most refractory patients, requiring the implantation of a permanent medical device. |
| • | Commercializing our therapy through traditional pharmaceutical channels. Our non-invasive delivery modality permits medical professionals to prescribe VNS through the same channel they would any other specialty medication. Refills delivered on a monthly basis enable us to seek widespread commercial payor coverage and reimbursement under a traditional pharmaceutical model. |
| • | Highly scalable and low investment manufacturing with digital refills. Our low manufacturing and assembly costs allow us to scale to meet demand with minimal additional investment. Refills through RFID or Bluetooth may offer attractive gross margins. |
| • | Potential for rapid label expansion in headache and regulatory approval in additional indications. In April 2017, the FDA cleared gammaCore for commercial sale in the United States and established a new therapeutic category: external vagal nerve stimulator for the treatment of headache. Through an expedited pathway, gammaCore received clearance for the acute treatment of pain associated with migraine in January 2018. We believe a similar regulatory pathway may be available to us for additional indications in rheumatology. |
| • | Broad intellectual property protection. Among our key issued patents, we have coverage on using our high-frequency burst signal for treating medical conditions until 2031, the low-pass filtering of that signal to ensure safe and comfortable transmission through the skin until 2031, the non-invasive treatment of headache conditions until 2029, and the remote network-enabled communication for the delivery of neuromodulation therapies for a broad range of conditions until 2033. |
| • | Highly experienced management team. Our management team includes executives with significant experience in the pharmaceutical and medical device industries, including positions at Pfizer, Merck, Novartis, Stryker and Zimmer Biomet. Members of our team have been involved in the launch and marketing of products including Motrin, Celebrex, and the migraine drugs Axert and Maxalt. Our team’s pharmaceutical experience in clinical development, sales, marketing and reimbursement, and its medical device experience in research, development and regulatory affairs, allow us to pursue our strategy and growth plans. |
2
Table of Contents
gammaCore Headache Pipeline
The following table summarizes our headache-related areas of focus for gammaCore:

| 1. | The gammaCore product registry for the acute treatment of cluster headache constitutes our initial commercialization efforts for our product. The full product launch is expected in the second quarter of 2018. |
Migraine
Migraine is a debilitating primary headache condition characterized by severe throbbing pain or a pulsing sensation, usually on one side of the head. Migraine affects approximately 12% of the adult population globally and disproportionately impacts women of childbearing years. In the United States, there are approximately 36 million migraine sufferers. Medications used to treat migraine include triptans, ergotamines, and anti-epileptic medications. Despite the fact that neurologists recognize the limited efficacy of, and the potential for abuse associated with, opioids, this class of medication continues to be prescribed for migraine at high rates, particularly in emergency departments. According to the U.S. Pharmacist, a leading pharmacy publication, upwards of 60% of the migraine patient population is dissatisfied with, or has contraindications to, the current standard of care migraine treatments. We estimate the addressable market for the acute treatment of migraine in the United States in 2018 will be approximately $3.8 billion. Five million migraine sufferers are treated annually by approximately 1,100 U.S. headache specialists, primarily neurologists.
Our FDA clearance for the acute treatment of migraine is principally supported by our pivotal trial, PRESTO. Statistical significance was achieved for complete pain relief at 30 minutes (gammaCore, 12.7%; sham, 4.2%; p=0.01), and maintained at 60 minutes (gammaCore, 21.0%; sham, 10.0%; p=0.02). The primary endpoint of PRESTO was pain-freedom at 120 minutes. While this trial did not reach statistical significance with respect to its primary endpoint, a repeated-measures test examined the inconsistency between the 120-minute finding and the 30- and 60-minute findings. This test demonstrated the statistical significance of gammaCore’s superiority over sham for the pain-free outcome through 120 minutes (gammaCore, 30.4%; sham, 19.7%; p=0.01). No serious adverse events were attributable to gammaCore in PRESTO, and the most commonly occurring adverse events were application site reactions, all of which were mild, transient, and tended to be self-limiting in nature. Based on these findings, the FDA cleared gammaCore for the acute treatment of migraine in adults.
3
Table of Contents
Cluster Headache
Cluster headache is a series of relatively short but extremely painful headaches that has been described by patients and physicians as one of the most painful conditions in medicine. The suicide rate among these patients is 20 times the U.S. national average, leading to the condition being referred to as the “suicide headache.” There are approximately 350,000 cluster headache sufferers in the United States, approximately 225,000 of whom seek treatment each year primarily from the same headache specialists who treat migraine, and we estimate the total annual addressable U.S. market for the acute treatment of these patients in 2018 will be approximately $400 million. Prior to gammaCore, there was only one FDA-approved, commercially available acute cluster headache treatment, injectable sumatriptan, and according to a 2016 market research survey, 87% of respondents reported dissatisfaction with the then-available treatment options for cluster headache.
Our FDA clearance for the acute treatment of episodic cluster headache is supported by two pivotal trials: ACT 1 and ACT 2. The primary endpoints of these trials were pain reduction and pain freedom within 15 minutes of the onset of the attack, respectively. While neither trial reached statistical significance with respect to its primary endpoint in the combined episodic and chronic cluster headache populations, both trials reached statistical significance (p<0.01 in each trial) on the primary endpoint in their predefined analysis of the episodic cluster headache subpopulation. To further define the benefit of gammaCore for the acute treatment of episodic cluster headache, the data from ACT 1 and ACT 2 were pooled to assess the overall response to each trial’s primary endpoint. Results of this pooled analysis reached statistical significance for the proportion of patients achieving mild or pain-free status at 15 minutes for the first attack (p<0.01 for the pooled data) and for the proportion of all treated attacks reaching pain freedom at 15 minutes (p<0.01 for the pooled data). No serious adverse events were attributable to gammaCore in ACT 1 or ACT 2. The most commonly occurring adverse events were application site reactions, all of which were mild, transient, and tended to be self-limiting in nature. Based on these findings, the FDA cleared gammaCore for the acute treatment of episodic cluster headache in adults.
Important advantages of gammaCore over other acute treatments for migraine and episodic cluster headache include its ease of use and suitability to be applied for as many attacks as a patient experiences per day, without the frequency-of-use restrictions and contraindications associated with other treatments.
Our Strategy
Our goal is to be a leader in bioelectronic medicine by using our proprietary non-invasive VNS platform therapy to deliver better patient outcomes. The key elements of our strategy include:
| • | Drive acceptance of our gammaCore products as a leading headache therapy, introducing it in cluster headache and expanding into migraine. We plan to establish gammaCore as the first-line treatment for episodic cluster headache patients, who have few alternative treatment options available to them. We will then leverage this position to expand into the broader headache market for migraine in the second quarter of 2018. |
| • | Drive reimbursement of our therapy. We are actively engaging with over 50 national and regional commercial insurance payors in the United States with the goal of securing reimbursement coverage as a pharmacy benefit. |
| • | Build a leading commercial presence. We have established a robust commercial capacity, including a specialty distribution channel with a concierge service to quickly onboard patients and manage payor interactions, and a direct sales force to target high prescribing neurology specialists and headache centers. |
4
Table of Contents
| • | Rapidly advance our pipeline. In 2018, we expect to initiate pivotal trials to support potential label expansion in headache, including additional trials in migraine prevention and migraine in adolescents. In 2018, we also expect to initiate our first major trials in rheumatology, including pivotal trials in Sjôgren’s syndrome and rheumatoid arthritis. Over the next 24 months, we anticipate additional sponsored pilot trials will be conducted in both neurology and rheumatology. |
Rheumatology Pipeline
Modulation of the peripheral immune system by VNS provides mechanistic support for the study of gammaCore in the treatment of inflammatory disorders. The systemic anti-inflammatory effects of VNS are believed to result from the activation of nerve fibers that release norepinephrine, causing specialized immune cells to release acetylcholine. This acetylcholine release activates a receptor on other immune cells, which blocks the pathways that promote inflammation. Based on initial positive results from our pilot trials, in 2018 we expect to initiate a series of pivotal trials designed to support regulatory approvals in multiple rheumatologic conditions, including Sjôgren’s syndrome and rheumatoid arthritis.
Manufacturing
We are the FDA-registered manufacturer of our gammaCore products, and we currently have sufficient capacity to meet anticipated demand for our therapy for the foreseeable future. We rely upon third-party suppliers, located both within and outside the United States, for substantially all of the component parts of gammaCore, including injection molded housings, printed circuit board assemblies, batteries, electrodes and conductive gel. We assemble, program and package our gammaCore products at our Basking Ridge, NJ facility and ship them into our distribution network.
The generation of our proprietary signal does not require custom electronic components. Therefore, we believe long-term supply agreements with our suppliers are not necessary as all the components used in our products are either high-volume, non-custom commodity components, or are readily available from multiple vendors. In cases where single sources exist, we have purchased such components with sufficient reserves to permit continued production of our product should simple design modifications be required.
Commercialization
We believe the significant unmet need and highly-targeted market of episodic cluster headache represents an ideal entry point for our therapy into the headache market, providing an opportunity to gain relevance with treating clinicians in order to support an expansion into migraine. Our commercial strategy will initially focus on the following priorities:
| • | Drive advocacy of gammaCore as a leading headache therapy. Our strategy is to establish gammaCore as a preferred treatment option, initially in episodic cluster headache and expanding into migraine. We are developing advocacy for gammaCore among key opinion leaders through our clinical program and initial product registry. We currently have in excess of 250 clinicians trained on gammaCore use. Of these, 50 are key opinion leaders who will lead a series of training and educational programs to advocate for gammaCore use among their colleagues |
| • | Drive reimbursement of our therapy. Through our product registry we are generating prescriptions and patient claims to prompt commercial payors to initiate reimbursement policies for gammaCore. We have engaged over 50 national and regional commercial insurance payors in the United States with the goal of obtaining reimbursement coverage as a pharmacy benefit. gammaCore currently has such pharmacy reimbursement coverage for |
5
Table of Contents
| 2.1 million commercial lives. Access negotiations have entered the active clinical review stage with more than a dozen additional insurance plans covering approximately 120 million additional commercial lives. |
| • | Build a leading commercial presence. We have partnered with an established specialty pharmacy network to provide physician and patient support to onboard patients and manage payor interactions. This support includes adjudication of all gammaCore prescriptions, payor claims for reimbursement, and patient support and training. Our sales force targets high-prescribing U.S. neurology practices and headache centers. We currently have a sales force of 17, with four medical science liaisons. We plan to hire an additional 19 territory business managers, who will ultimately cover 6,000 high-prescribers of headache medications. |
Risks Associated with our Business
Our business is subject to a number of risks and uncertainties you should be aware of before making an investment decision. These risks are discussed more fully in the “Risk Factors” section immediately following this prospectus summary. These risks include the following:
| • | We have a history of significant losses. If we do not achieve and sustain profitability, our financial condition could suffer. |
| • | We will be required to obtain additional funds in the future, and these funds may not be available on acceptable terms or at all. |
| • | If third-party payors do not provide adequate coverage and reimbursement for gammaCore, our business will be negatively impacted. |
| • | Third-party payors may not agree to cover gammaCore through pharmacy benefit plans, which will hinder our commercialization strategy and require changes to our existing business that could delay and negatively impact our ability to generate net sales. |
| • | We must demonstrate to physicians the merits of our gammaCore therapy compared to those of our competitors. |
| • | We only recently began commercializing gammaCore in the United States and we may never achieve market acceptance. |
| • | Our business is subject to extensive governmental regulation that makes it expensive and time consuming for us to bring our gammaCore therapy to market in the United States and to expand the use of our gammaCore therapy to additional therapeutic indications. |
| • | Clinical trials are very expensive, time-consuming and difficult to design and implement and involve uncertain outcomes. Furthermore, results of earlier preclinical studies and clinical trials may not be predictive of results of future preclinical studies or clinical trials. |
| • | If our competitors are better able to develop and market treatments that are safer, more effective, less costly, easier to use or otherwise more attractive than gammaCore, our business will be adversely impacted. |
| • | We rely upon third-party, and in certain cases single-source suppliers for many of the components and materials used in manufacturing gammaCore, and for critical manufacturing and packaging services, making us vulnerable to supply shortages and problems and price fluctuations, which could harm our business. |
| • | We rely on a variety of intellectual property rights, and if we are unable to maintain or protect our intellectual property, our business and results of operations will be harmed. |
6
Table of Contents
| • | Our principal stockholders and management own a significant percentage of our stock and will be able to exert significant control over matters subject to stockholder approval. |
Corporate Conversion
We currently operate as a Delaware limited liability company under the name Electrocore, LLC. Prior to the closing of this offering, Electrocore, LLC will convert into a Delaware corporation pursuant to a statutory conversion and change its name to electroCore, Inc. As a result of the corporate conversion, the holders of the different classes and series of units of Electrocore, LLC, or Units, and warrants to purchase Units, will become holders of common stock of electroCore, Inc. and, for certain holders, options to purchase our common stock. The number of shares of our common stock, options to purchase our common stock, and warrants to purchase our common stock that holders of Units and warrants to purchase Units will be entitled to receive in the corporate conversion will be determined in accordance with the plan of conversion and our Third Amended and Restated Limited Liability Company Agreement, dated November 21, 2017, or the Operating Agreement, and varies depending on which class and series of Units a holder owns, and the terms of the applicable warrants. The number of shares of common stock certain holders of our Units will receive in connection with the corporate conversion will also vary depending on the initial public offering price set forth on the cover page of this prospectus. See “Corporate Conversion.”
The information in this prospectus is based on our estimate that, in the corporate conversion, shares of our common stock will be issued to holders of Units, warrants to purchase shares of common stock will be issued to holders of warrants to purchase Units, and options to purchase shares of our common stock will be issued to certain holders of Units that were originally issued as profits interests, in each case, based on an initial public offering price per share of common stock of $ , which is the midpoint of the price range set forth on the cover page of this prospectus. To the extent that the actual initial public offering price per share for this offering is greater or less than $ , the actual number of shares of common stock, options and warrants to be issued in connection with the conversion will be adjusted accordingly. Unless the context otherwise requires, and as further described below in “Corporate Conversion,” references to Units exclude Units originally issued as profits interests.
The purpose of the corporate conversion is to reorganize our corporate structure so that the entity that is offering our common stock to the public in this offering is a corporation rather than a limited liability company and so that our existing investors will own our common stock rather than equity interests in a limited liability company. For further information regarding the corporate conversion, see “Corporate Conversion.” References in this prospectus to our capitalization and other matters pertaining to our equity and shares prior to the corporate conversion relate to the capitalization and equity and shares of Electrocore, LLC, and after the corporate conversion, to electroCore, Inc.
Implications of Being an Emerging Growth Company
We are an “emerging growth company” as defined in the Jumpstart Our Business Startups Act of 2012, or the JOBS Act, which permits us to elect not to be subject to certain disclosure and other requirements that otherwise would have been applicable to us had we not been an “emerging growth company.” These provisions include:
| • | only two years of audited financial statements, in addition to any required unaudited interim financial statements, with correspondingly reduced “Management’s Discussion and Analysis of Financial Condition and Results of Operations” disclosure in this prospectus; and |
| • | reduced disclosure about our executive compensation arrangements; |
7
Table of Contents
| • | no non-binding advisory votes on executive compensation or golden parachute arrangements; and |
| • | exemption from the auditor attestation requirement in the assessment of our internal control over financial reporting. |
We may take advantage of these exemptions for up to five years or such earlier time as we are no longer an “emerging growth company.” We will qualify as an “emerging growth company” until the earliest of (1) the last day of our fiscal year following the fifth anniversary of the date of completion of this offering, (2) the last day of our fiscal year in which we have annual gross revenue of $1.07 billion or more, (3) the date on which we have, during the previous three-year period, issued more than $1.0 billion in non-convertible debt and (4) the last day of the fiscal year in which we become a “large accelerated filer” as defined in Rule 12b-2 under the Securities Exchange Act of 1934, as amended, or the Exchange Act. Under this definition, we will be an “emerging growth company” upon completion of this offering and could remain an “emerging growth company” until as late as December 31, 2023.
In addition, the JOBS Act provides that an emerging growth company can take advantage of an extended transition period for complying with new or revised accounting standards. This allows an emerging growth company to delay the adoption of certain accounting standards until those standards would otherwise apply to private companies. We have irrevocably elected not to avail ourselves of this exemption from new or revised accounting standards and, therefore, we will comply with new or revised accounting standards when they are required to be adopted by other public companies that are not emerging growth companies.
Corporate Information
Electrocore, LLC was established in Delaware in September 2005. Prior to the closing of this offering, we will complete a corporate conversion pursuant to which electroCore, Inc. will succeed to the business of Electrocore, LLC and its consolidated subsidiaries, and the equity holders of Electrocore, LLC will become stockholders, option holders and warrant holders of electroCore, Inc. See “Corporate Conversion.” Our principal executive offices are located at 150 Allen Rd., Suite 201, Basking Ridge, New Jersey 07920, and our telephone number at that address is (973) 290-0097. Our website is located at www.electrocore.com. Our website, and the information on our website, is neither part of this prospectus nor incorporated by reference herein.
8
Table of Contents
| Common stock offered by us |
shares. | |
| Common stock to be outstanding after this offering |
shares (or shares if the underwriters’ option to purchase additional shares is exercised in full). | |
| Underwriters’ option to purchase additional shares of common stock from us |
We have granted the underwriters a 30-day option to purchase an additional shares. | |
| Use of proceeds |
We estimate, based upon an assumed initial public offering price of $ per share, which is the midpoint of the price range set forth on the cover page of this prospectus, we will receive proceeds from the offering of approximately $ million (or $ million if the underwriters’ option to purchase additional shares is exercised in full), after deducting estimated underwriting discounts and commissions and estimated offering expenses payable by us. We intend to use the proceeds from this offering for working capital and other corporate purposes including to (i) continue funding our activities related to the commercial launch of gammaCore, initially for the acute treatment of migraine and episodic cluster headache in the United States, (ii) invest in the expansion of gammaCore into additional indications in headache and rheumatology, and (iii) further build out our specialty distribution channel for gammaCore Sapphire. See “Use of Proceeds.” | |
| Risk factors |
You should carefully read and consider the information set forth under the heading “Risk Factors” beginning on page 13 of this prospectus and all other information set forth in this prospectus before investing in our common stock. | |
| Proposed Nasdaq Global Select Market symbol |
“ECOR” | |
The common stock to be outstanding after this offering is based on shares outstanding as if the corporate conversion had been effected as of , 2018, and excludes the following:
| • | shares issuable upon the exercise of options outstanding as of , 2018 at an exercise price equal to the initial public offering price of $ per share, which is the midpoint of the price range set forth on the cover page of this prospectus, following the corporate conversion; |
| • | shares issuable upon the exercise of warrants outstanding as of , 2018 at a weighted-average exercise price of $ per share following the corporate conversion; |
| • | shares of common stock reserved for issuance pursuant to future awards under our 2018 Omnibus Equity Incentive Plan, or the 2018 Plan, which will become effective immediately prior to the consummation of this offering; and |
9
Table of Contents
| • | the issuance of shares of common stock in satisfaction of $3,629,092 in respect of an accrued but unpaid preference to holders of our Series A Preferred Units (which may be paid in cash or such shares, at our option). |
Unless otherwise indicated, this prospectus assumes:
| • | the completion of our corporate conversion, as a result of which Units will be converted into shares of common stock of electroCore, Inc., warrants to purchase Units will be converted into the right to purchase shares of common stock of electroCore, Inc., and Units that were originally issued as profits interests will be converted into shares of our common stock and, with respect to such Units held by persons who are our employees and consultants at the time of the conversion, options to purchase shares of common stock of electroCore, Inc., in each case, based on the assumed initial public offering price of $ per share, which is the midpoint of the price range set forth on the cover page of this prospectus; |
| • | an initial public offering price of $ per share, which is the midpoint of the estimated initial public offering price range set forth on the cover page of this prospectus; |
| • | no exercise of the outstanding options and warrants described above; and |
| • | no exercise of the underwriters’ option to purchase up to an additional shares of our common stock. |
The number of shares of common stock of electroCore, Inc. that holders of Units will receive in the corporate conversion and the number of shares of common stock that options and warrants will be exercisable for following the corporate conversion will vary depending on the initial public offering price.
10
Table of Contents
SUMMARY CONSOLIDATED FINANCIAL DATA
The following tables present summary consolidated financial data for our business. You should read this data together with our audited consolidated financial statements and related notes appearing elsewhere in this prospectus and the information under the captions “Selected Consolidated Financial Data,” “Capitalization” and “Management’s Discussion and Analysis of Financial Condition and Results of Operations.”
We derived the following consolidated statements of operations data for the years ended December 31, 2016 and 2017 and the following balance sheet data as of December 31, 2017 from our audited consolidated financial statements appearing elsewhere in this prospectus. Our historical results are not necessarily indicative of our future results.
| Year ended December 31, |
||||||||
| 2016 | 2017 | |||||||
| (in thousands, except unit and per unit amounts) |
||||||||
| Consolidated statements of operations: |
||||||||
| Net sales |
$ | 254.1 | ||||||
| Cost of goods sold |
123.7 | |||||||
|
|
|
|
|
|||||
| Gross profit |
130.4 | |||||||
| Operating expenses |
||||||||
| Research and development |
7,971.3 | |||||||
| Selling, general and administrative |
7,169.3 | |||||||
|
|
|
|
|
|||||
| Total operating expenses |
15,140.6 | |||||||
|
|
|
|
|
|||||
| Loss from operations |
(15,010.2 | ) | ||||||
| Amortization of debt discount and issuance costs |
536.9 | |||||||
| Interest expense |
234.4 | |||||||
|
|
|
|
|
|||||
| Net loss |
(15,781.5 | ) | ||||||
| Less Net loss attributable to noncontrolling interest |
(44.1 | ) | ||||||
|
|
|
|
|
|||||
| Net loss attributable to Electrocore, LLC, subsidiaries and affiliate |
$ | (15,737.4 | ) | |||||
|
|
|
|
|
|||||
| Pro forma net loss per unit data(1): |
||||||||
| Pro forma net loss per unit—basic and diluted (unaudited) |
||||||||
| Pro forma weighted average number of common units used to calculate loss per unit—basic and diluted (unaudited) |
||||||||
| (1) | We have presented pro forma basic and diluted net loss per unit for the year ended December 31, 2017, which consists of our historical net loss attributable to Electrocore LLC, subsidiaries and affiliate, divided by the pro forma basic and diluted weighted average number of shares of common stock outstanding after giving effect to the conversion of all of our outstanding Common Units, Series A Preferred Units and Series B Preferred Units into shares of our common stock prior to the closing of this offering. Net loss used in calculating net loss per unit does not reflect (i) the estimated expenses of this offering or (ii) compensation and expenses for our board of directors and other costs related to operating as a public company. For more information on how we calculate basic and diluted pro forma weighted average number of units outstanding, see Note 8 to our audited consolidated financial statements included elsewhere in this prospectus. The calculations described above do not give effect to the potential issuance of shares of common stock at the initial public offering price in satisfaction of $3,629,092 in respect of an accrued but unpaid preference to holders of our Series A Preferred Units (which may be paid in cash or such shares, at our option). |
11
Table of Contents
| As of December 31, 2017 | ||||||||||||
| (in thousands) | ||||||||||||
| Actual | Pro forma(1) | Pro forma as adjusted(2) |
||||||||||
| (unaudited) | ||||||||||||
| Consolidated balance sheet data: |
||||||||||||
| Cash and cash equivalents |
$ | $ | $ | |||||||||
| Working capital(3) |
||||||||||||
| Total assets |
||||||||||||
| Long-term debt |
||||||||||||
| Series A Preferred Units |
||||||||||||
| Series B Preferred Units |
||||||||||||
| Common Units |
||||||||||||
| Total members’/stockholders’ equity (deficit) |
||||||||||||
| (1) | Pro forma to reflect our conversion from a Delaware limited liability company to a Delaware corporation prior to the closing of this offering, in which all outstanding Units of Electrocore, LLC will be converted into shares of common stock of electroCore, Inc. at an assumed initial public offering price of $ per share, which is the midpoint of the price range set forth on the cover page of this prospectus. The number of shares of common stock of electroCore, Inc. that holders of Units will receive in the corporate conversion and the number of shares of common stock that options and warrants will be exercisable for following the corporate conversion will vary depending on the initial public offering price. |
| (2) | Pro forma as adjusted gives further effect to the sale of shares of our common stock in this offering at an assumed initial public offering price of $ per share, which is the midpoint of the price range set forth on the cover page of this prospectus, after deducting the estimated underwriting discounts and commissions and estimated offering expenses payable by us and the application of the proceeds therefrom. |
| (3) | We define working capital as current assets less current liabilities. |
12
Table of Contents
Investing in our common stock involves a high degree of risk. You should carefully consider the risks and uncertainties described below, together with all of the other information in this prospectus, including our consolidated financial statements and related notes, before investing in our common stock. The risks and uncertainties described below are not the only ones we face. Additional risks and uncertainties that we are unaware of, or that we currently believe are not material, may also become important factors that affect us. If any of the following risks occur, our business, operating results and prospects could be materially harmed. In that event, the price of our common stock could decline, and you could lose part or all of your investment.
Risks Related to our Financial Position, Operating Results and Need for Additional Capital
We have a history of significant losses. If we do not achieve and sustain profitability, our financial condition could suffer.
We have experienced significant net losses, and we expect to continue to incur losses for the foreseeable future as we seek to grow our sales and marketing infrastructure, to increase market acceptance of our gammaCore therapy for the acute treatment of episodic cluster headache, or eCH, and the acute treatment of migraine, fund our research and development activities, to expand our manufacturing capabilities, and to obtain regulatory clearance or approval for other products or indications in the United States and internationally. We incurred a net loss of $ million for the year ended December 31, 2017. As of December 31, 2017, our accumulated deficit was $ million. Our prior losses, combined with expected future losses, have had and will continue to have, for the foreseeable future, an adverse effect on our stockholders’ deficit and working capital.
To become and remain profitable, we must successfully commercialize our gammaCore therapy and continue to identify promising new areas of treatment with significant market potential. This will require us to be successful in a range of challenging activities, including completing clinical trials of gammaCore for additional therapeutic indications, developing commercial scale manufacturing processes, obtaining additional marketing clearance or approval from regulatory authorities, obtaining adequate coverage and reimbursement from payors, manufacturing, marketing and selling any current and future product candidates for which we may obtain marketing clearance or approval, and satisfying any post-marketing requirements. We may never succeed in any or all of these activities and, even if we do, we may never generate sufficient revenue to achieve profitability.
Even if we do achieve profitability, we may not be able to sustain or increase profitability in subsequent periods. Our failure to become and remain profitable would decrease the value of our company and could impair our ability to raise capital, maintain our research and development efforts, expand our business or continue our operations. A decline in the value of our company also could cause you to lose all or part of your investment.
We will be required to obtain additional funds in the future, and these funds may not be available on acceptable terms or at all.
Our operations have consumed substantial amounts of cash since inception, and we anticipate our expenses will increase as we expand our commercial sales force in the United States, investigate the use of our gammaCore therapy for the treatment of additional new indications, including Sjôgren’s syndrome and rheumatoid arthritis, and continue to grow our business and transition to operating as a public company. We believe that our growth will depend, in part, on our ability to fund our efforts to commercialize our gammaCore therapy for the acute treatment of eCH and the acute treatment of migraine, and to pursue research and development activities for additional indications for our gammaCore therapy. Our existing resources may not allow us to conduct all of the activities that we believe would be beneficial for our future growth. As a result, we may need to seek additional funds in
13
Table of Contents
the future. If we are unable to raise funds on favorable terms, or at all, we may not be able to support our commercialization efforts or increase our research and development activities and the growth of our business may be negatively impacted. As a result, we may be unable to compete effectively. For the year ended December 31, 2016, our net cash used in operating activities was $13.2 million, and as of December 31, 2017 our working capital was $ million, which included $ million in cash and cash equivalents, as well as $ million in short-term investments. We expect that our existing cash, together with the net proceeds from this offering, will enable us to fund our operating expenses and capital expenditure requirements through at least the next 12 months. This estimate is based on assumptions that may prove to be wrong, and we could exhaust our available capital resources sooner than we expect. Changes, including those relating to our development activities and regulatory matters, may occur beyond our control that would cause us to consume our available capital more quickly. Our future capital requirements will depend on many factors, including:
| • | the outcome, timing of, and costs involved in, seeking and obtaining clearances or approvals from the FDA and other regulatory authorities, including the potential for the FDA and other regulatory authorities to require that we perform more studies, clinical trials or tests on our gammaCore therapy than we currently expect; |
| • | the scope and timing of our investment in our U.S. commercial infrastructure and sales force; |
| • | the research and development activities we intend to undertake in order to expand our headache indications and enhancements to our gammaCore therapy that we intend to pursue; |
| • | the costs of commercialization activities including sales, marketing, manufacturing and distribution; |
| • | the degree and rate of market acceptance of our gammaCore therapy; |
| • | the costs of filing, prosecuting, defending and enforcing any patent claims and other intellectual property rights; |
| • | our need to implement additional infrastructure and internal systems; |
| • | our ability to hire additional personnel to support our operations as a public company; and |
| • | the emergence of competing therapies or other adverse market developments. |
To finance these activities, we may seek funds through borrowings or through additional rounds of financing, including private or public equity or debt offerings and collaborative arrangements with corporate partners. We may be unable to raise funds on favorable terms, if at all.
The sale of additional equity or convertible debt securities could result in additional dilution to our stockholders. If we borrow additional funds or issue debt securities, lenders or security holders could have rights superior to holders of our common stock and such indebtedness could contain covenants that will restrict our operations. We might have to obtain funds through arrangements with collaborative partners or others that may require us to relinquish rights to our technologies, therapeutic candidates, or products that we otherwise would not relinquish. If we do not obtain additional resources, our ability to capitalize on business opportunities will be limited, we may be unable to compete effectively and the growth of our business will be harmed.
If third-party payors do not provide adequate coverage and reimbursement for the use of gammaCore, we will be unable to generate significant revenues.
Our success in marketing and commercializing gammaCore depends and will depend in large part on whether U.S. and international government health administrative authorities, private health insurers and other payor organizations provide adequate coverage and reimbursement for the cost of our products.
14
Table of Contents
Many third-party payors do not currently cover VNS for any indications other than epilepsy because they have determined all other VNS modalities to be investigational or experimental. If physicians or insurers do not find our clinical data compelling or wish to wait for additional studies, they may choose not to use or provide coverage and reimbursement for gammaCore. We cannot provide assurance that data we or others may generate in the future will be consistent with that observed in our existing clinical studies, or that our current or future published clinical evidence will be sufficient to obtain adequate coverage and reimbursement for our products.
In the United States, we expect to derive nearly all of our sales from prescriptions of gammaCore from neurologists and primary care physicians. Access to adequate coverage and reimbursement by third-party payors for treatment of cluster and migraine headaches using our gammaCore therapy is essential to the acceptance of our products by customers and patients, because without such coverage and reimbursement, customers and patients will have to be willing to bear the entire cost of our therapy.
Third-party payors, whether foreign or domestic, or governmental or commercial, are developing increasingly sophisticated methods of controlling healthcare costs. In addition, in the United States, no uniform policy of coverage and reimbursement for our gammaCore therapy exists among third-party payors. Therefore, coverage and reimbursement for our gammaCore therapy can differ significantly from payor to payor. In addition, payors continually review new technologies for possible coverage and can, without notice, deny coverage for these new products and procedures. As a result, the coverage determination process is often a time-consuming and costly process that will require us to provide scientific and clinical support for the use of our gammaCore therapy to each payor separately, with no assurance that coverage and adequate reimbursement will be obtained, or maintained if obtained.
Reimbursement systems in international markets vary significantly by country and by region within some countries, and reimbursement approvals must be obtained on a country-by-country basis. In many international markets, a product must be approved for reimbursement before it can be approved for sale in that country. Further, many international markets have government-managed healthcare systems that control reimbursement for new devices and procedures. In most markets, there are private insurance systems as well as government-managed systems. If sufficient and timely coverage and reimbursement is not available for our current or future products, in either the United States or internationally, the demand for our products and our revenues will be adversely affected.
Third-party payors may not agree to cover gammaCore through pharmacy benefit plans, which will hinder our commercialization strategy and require changes to our existing business that could delay and negatively impact our ability to generate revenue.
Our commercialization strategy in the United States advocates for coverage and reimbursement for gammaCore under payors’ pharmacy benefit. Third-party payors, including government health programs and private insurers, may not be willing or able to cover gammaCore under pharmacy benefit plans, which are often limited to coverage of prescription drug products. For example, Medicare’s voluntary pharmacy benefit, Medicare Part D, limits coverage under this benefit to prescription drugs, biologicals, and supplies used in the delivery of insulin, but does not cover medical devices like gammaCore or its supplies.
To obtain coverage and reimbursement from Medicare and any other third-party payor that will not cover gammaCore under a pharmacy benefit, we may be required to seek coverage and reimbursement as a medical device or item of durable medical equipment. Obtaining coverage under an alternative benefit model may require us to modify our commercialization strategy, our distribution model, our pricing, our
15
Table of Contents
products, and our operations. If needed to obtain third-party payor coverage and reimbursement under an alternative benefit, these potential changes may entail numerous risks, including increased operating expenses, requirements to comply with healthcare regulatory laws, the loss of or delay in obtaining revenue, and uncertainty in our ability to successfully implement the modifications. The failure to obtain recognition by third-party payors under the pharmacy benefit model could have a material adverse effect on the sales of gammaCore and the results of our operations.
We must demonstrate to physicians the merits of our gammaCore therapy compared to those of our competitors.
Physicians play a significant role in determining the course of a patient’s treatment and, as a result, the type of product that will be used to treat a patient. As a result, our success depends, in large part, on effectively marketing our gammaCore therapy to physicians. In order for our gammaCore therapy to gain widespread adoption, we must successfully demonstrate to physicians the merits of our gammaCore therapy for the acute treatment of eCH and the acute treatment of migraine, compared to our competitors’ products, including products being developed by Allergan, Amgen, Biohaven, Eli Lilly, Novartis and Teva, for use in treating patients with cluster and migraine headaches, particularly because noninvasive VNS, or nVNS, is relatively new as compared to existing traditional treatments for cluster and migraine headaches. Acceptance of our gammaCore therapy depends on educating physicians as to the distinctive characteristics, perceived benefits, safety, ease of use and cost-effectiveness of our gammaCore therapy as compared to our competitors’ products, and communicating to physicians the proper use of our gammaCore therapy. If we are not successful in convincing physicians of the merits of our gammaCore therapy or educating them on the benefits of our gammaCore therapy, they may not prescribe our gammaCore therapy and we may be unable to increase our sales, sustain our growth or achieve profitability. In addition, we believe support of our products by physicians is essential for market acceptance and adoption. If we do not receive support from physicians or long-term data does not show the benefits of using our gammaCore therapy, physicians may not use it. In such circumstances, our results of operations would be materially adversely affected.
Our operating results may vary significantly from quarter to quarter because of seasonality or otherwise.
Our quarterly revenue and results of operations may fluctuate from quarter to quarter due to, among others, the following reasons:
| • | physician and payor acceptance of our gammaCore therapy; |
| • | the timing, expense and results of research and development activities, clinical trials and regulatory clearance or approvals; |
| • | fluctuations in our expenses associated with expanding our commercial operations and operating as a public company; |
| • | the introduction of new products, therapies and technologies by competitors; |
| • | the productivity of our sales representatives; |
| • | supplier, manufacturing or quality problems with our products; |
| • | the timing of stocking orders from our distributors; |
| • | changes in our pricing policies or in the pricing policies of our competitors or suppliers; and |
| • | adverse developments in coverage amounts or government and third-party payors’ reimbursement policies. |
Our results may also fluctuate on a seasonal basis due to the seasonality of cluster and migraine headache attacks, which could affect the comparability of our results between periods. These seasonal
16
Table of Contents
variations are difficult to predict accurately, may vary across different markets, and at times may be entirely unpredictable, which introduces additional risk into our business as we may rely upon forecasts of customer demand to build inventory in advance of anticipated sales. In addition, we believe our limited history commercializing our gammaCore therapy has, in part, made our seasonal patterns more difficult to discern, making it more difficult to predict future seasonal patterns.
Because of these and other factors, it is likely that in some future period our operating results will not meet investor expectations or those of public market analysts.
Any unanticipated change in revenues or operating results is likely to cause our stock price to fluctuate. New information may cause investors and analysts to revalue our business, which could cause a decline in our stock price.
Failure to protect our information technology infrastructure against cyber-based attacks, network security breaches, service interruptions, or data corruption could significantly disrupt our operations and adversely affect our business and operating results.
We rely on information technology and telephone networks and systems, including the internet, to process and transmit sensitive electronic information and to manage or support a variety of business processes and activities, including sales, billing, marketing, procurement and supply chain, manufacturing, and distribution. We also rely on information technology systems to support our proprietary data warehouse, which, among other things, maintains patient product serial numbers and allows for prescription refills at specialty pharmacies through RFID cards. In addition, we use enterprise information technology systems to record, process, and summarize financial information and results of operations for internal reporting purposes and to comply with regulatory, financial reporting, legal, and tax requirements. Our information technology systems, some of which are managed by third-parties, and the information technology systems of third parties may be susceptible to damage, disruptions, or shutdowns due to computer viruses, attacks by computer hackers, failures during the process of upgrading or replacing software, databases or components thereof, power outages, hardware failures, telecommunication failures, user errors, or catastrophic events. Despite the precautionary measures we and third parties have taken to prevent breakdowns in information technology and telephone systems, if these systems are breached or suffer severe damage, disruption, or shutdown and we are unable to effectively resolve the issues in a timely manner, our business and operating results may suffer and we may be subject to related lawsuits.
We may engage in future acquisitions that increase our capital requirements, dilute our stockholders, cause us to incur debt or assume contingent liabilities and subject us to other risks.
We may evaluate various strategic transactions, including licensing or acquiring complementary therapies, products, technologies or businesses. Any potential acquisitions may entail numerous risks, including increased operating expenses and cash requirements, assimilation of operations and products, retention of key employees, diversion of our management’s attention and uncertainties in our ability to maintain key business relationships of the acquired entities. In addition, if we undertake acquisitions, we may issue dilutive securities, assume or incur debt obligations, incur large one-time expenses and acquire intangible assets that could result in significant future amortization expense. Moreover, we may not be able to locate suitable acquisition opportunities and this inability could impair our ability to grow or obtain access to technology or products that may be important to the development of our business.
17
Table of Contents
Risks Related to Our Business and the Development of Our gammaCore Therapy
Our business is subject to extensive governmental regulation that makes it expensive and time consuming for us to bring our gammaCore therapy to market in the United States and to expand the use of our gammaCore therapy to additional therapeutic indications.
Our gammaCore therapy must comply with regulatory requirements imposed by the FDA in the United States and similar agencies in foreign jurisdictions. These requirements involve lengthy and detailed laboratory and clinical testing procedures, sampling activities, extensive agency review processes, and other costly and time-consuming procedures. It often takes several years to satisfy these requirements, depending on the complexity and novelty of the product. We also are subject to numerous additional licensing and regulatory requirements relating to safe working conditions, manufacturing practices, environmental protection, fire hazard control, and disposal of hazardous or potentially hazardous substances. Some of the most important requirements we must comply with include:
| • | the Federal Food, Drug, and Cosmetic Act and the FDA’s implementing regulations (Title 21 CFR); |
| • | CE mark requirements of the European Union, or EU; |
| • | Medical Device Quality Management System Requirements (ISO 13485:2003); |
| • | Occupational Safety and Health Administration requirements; and |
| • | New Jersey Department of Health Services requirements. |
Government regulation may impede our ability to conduct clinical trials and to manufacture and sell our existing therapy and any future products. Government regulation also could delay our marketing of new products for a considerable period of time and impose costly procedures on our activities. The FDA and other regulatory agencies may not clear or approve our gammaCore therapy in additional therapeutic areas that we may pursue, including Sjôgren’s syndrome and rheumatoid arthritis, on a timely basis, if at all. Any delay in obtaining, or failure to obtain, such clearances or approvals could negatively impact our marketing of our gammaCore therapy and impede our ability to bring future products to market.
Our gammaCore therapy will remain subject to strict regulatory controls on manufacturing, marketing and use. We may be forced to modify or recall a product after release in response to regulatory action or unanticipated difficulties encountered in general use. Any such action could have a material effect on the reputation of our gammaCore therapy and on our business and financial position.
Further, regulations may change, and any additional regulation could limit or restrict our ability to use any of our technologies, which could harm our business. We could also be subject to new international, federal, state or local regulations that could affect our research and development programs and harm our business in unforeseen ways. If this happens, we may have to incur significant costs to comply with such laws and regulations, which will harm our results of operations.
We may in the future become involved in lawsuits to protect or enforce our intellectual property, which could be expensive and time consuming, and ultimately unsuccessful, and could result in the diversion of significant resources, thereby hindering our ability to effectively commercialize our existing or future products. If we are unable to obtain, maintain, protect, and enforce our intellectual property, our business will be negatively affected.
The markets in which we compete and expect to compete are subject to rapid technological change and frequent litigation regarding patent and other intellectual property rights. It is possible that our patents or licenses may not withstand challenges made by others or protect our rights adequately.
Our success depends in large part on our ability to secure effective patent protection for our products and processes in the United States and internationally. We have filed and intend to continue to file patent
18
Table of Contents
applications for various aspects of our technology and trademark applications to protect our brand and business, and copyright applications to protect our software. We seek to obtain and maintain patents and other intellectual property rights to restrict the ability of others to market products or services that misappropriate our technology and work product and/or infringe our intellectual property to compete with our products and services.
However, we face the risks that:
| • | We may fail to secure necessary patents, potentially permitting competitors to market competing products and services and make, use or sell products or offer services that are substantially the same as ours without incurring the sizeable development costs that we have incurred, which would adversely affect our ability to compete. |
| • | Patents may not issue from any of our currently pending or future patent applications. |
| • | Our already-granted patents and any future patents may not survive legal challenges to their scope, validity or enforceability, or provide significant protection for us, and they may be challenged in a post grant review or inter partes review proceeding, re-examined or invalidated, and/or may be found to be unenforceable or not cover competing processes, products or services. |
| • | Even if our patents are determined by the U.S. Patent and Trademark Office, or USPTO, foreign patent office, or a court to be valid and enforceable, they may not be drafted or interpreted sufficiently broadly to prevent others from marketing products and services similar to ours or designing around our patents. For example, third parties may be able to develop therapies, or make systems or devices, that are similar to ours but that are not covered by the claims of our patents. Third parties may assert that we or our licensors were not the first to make the inventions covered by our issued patents or pending patent applications. The claims of our issued patents or patent applications when issued may not cover our commercial technology or the future products and services that we develop. We may not have freedom to operate unimpeded by the patent rights of others. Third parties may have dominating, blocking or other patents relevant to our technology of which we are not aware. In addition, because patent applications in the United States and many foreign jurisdictions are typically not published until 18 months after the filing of certain priority documents (or, in some cases, are not published until they issue as patents) and because publications in the scientific literature often lag behind actual discoveries, we cannot be certain that others have not filed patent applications for our technology or our contemplated technology. Any such patent applications may have priority over our patent applications or issued patents, which could further require us to obtain rights from third parties to issued patents or pending patent applications covering such technologies to allow us to commercialize our technology. If another party has filed a U.S. patent application on inventions similar to ours, depending on when the timing of the filing date falls under certain patent laws, we may have to participate in a priority contest (such as an interference proceeding) declared by the USPTO to determine priority of invention in the United States. There may be prior public disclosures of which we are not aware that could invalidate our patents or a portion of the claims of our patents. Further, we may not develop additional proprietary technologies and, even if we do, they may not be patentable. |
| • | Patent law can be highly uncertain and involve complex legal and factual questions for which important principles remain unresolved. In the United States and in many foreign jurisdictions, policies regarding the breadth of claims allowed in patents can be inconsistent. The U.S. Supreme Court and the U.S. Court of Appeals for the Federal Circuit have made, and will likely continue to make, changes in how the patent laws of the United States are interpreted. Similarly, foreign courts have made, and will likely continue to make, changes in |
19
Table of Contents
| how the patent laws in their respective jurisdictions are interpreted. We cannot predict future changes in the interpretation of patent laws or changes to patent laws that might be enacted into law by U.S. and foreign legislative bodies. Those changes may materially affect our patents or patent applications, our ability to obtain patents, or the patents and patent applications of our licensors. Future protection for our proprietary rights is uncertain because legal means afford only limited protection and may not adequately protect our rights or permit us to gain or keep our competitive advantage, which could adversely affect our financial condition and results of operations. |
| • | Monitoring unauthorized uses of our intellectual property is difficult and costly. From time to time, we seek to analyze our competitors’ therapies, products and services, and may in the future seek to enforce our patents or other proprietary rights against potential infringement. However, the steps we have taken to protect our proprietary rights may not be adequate to prevent misappropriation of our intellectual property. We may not be able to detect unauthorized use of, or take appropriate steps to enforce, our intellectual property rights. Our competitors may also independently develop similar technology. Any inability to meaningfully protect our intellectual property could result in competitors offering products that incorporate our product features, which could reduce demand for our gammaCore therapy. In addition, we may need to defend our patents from third-party challenges, including interferences, derivation proceedings, re-examination proceedings, post-grant review, inter partes review, third-party submissions, oppositions, nullity actions, or other patent proceedings. We may need to initiate infringement claims or litigation. Adverse proceedings such as litigation can be expensive, time consuming and may divert the efforts of our technical and managerial personnel, which could in turn harm our business, whether or not we receive a determination favorable to us. In addition, in an infringement proceeding, a court may decide that the patent we seek to enforce is invalid or unenforceable, or may refuse to enjoin the other party from using the technology at issue on the grounds that the patent in question does not cover the technology in question. An adverse result in any litigation could place one or more of our patents at risk of being invalidated or interpreted narrowly. Some of our competitors may be able to devote significantly more resources to intellectual property litigation, and may have patent portfolios, including significantly broader patent portfolios, to assert against us, if we assert our rights against them. Further, because of the substantial discovery required in connection with intellectual property litigation, there is a risk that some of our confidential information could be disclosed or otherwise compromised during litigation. |
| • | We may not be able to accurately estimate or control our future operating expenses in relation to obtaining, enforcing and/or defending intellectual property, which could lead to cash shortfalls. Our operating expenses may fluctuate significantly in the future as a result of the costs of preparing, filing, prosecuting, defending and enforcing patent claims and other patent related costs, including litigation costs and the results of such litigation. |
| • | We may also be forced to enter into cross-license agreements with competitors in order to manufacture, use, sell, offer for sale, import and/or export products or services that are covered by our competitors’ intellectual property rights. If we need to use our intellectual property to enter such cross-license agreements, it may compromise the value of our intellectual property due to the fact that our competitors may be able to manufacture, use, sell, offer for sale, import and/or export our patented technology. |
For additional information regarding risks related to our intellectual property, see “—Risks Related to Intellectual Property.”
20
Table of Contents
If serious adverse events or other undesirable side effects are identified during the use of our gammaCore therapy in investigator-sponsored trials, it may adversely affect our development of such product candidates.
Undesirable side effects caused by our gammaCore therapy or future product candidates could cause us or regulatory authorities to interrupt, delay or halt nonclinical studies and clinical trials, or could make it more difficult for us to enroll patients in our clinical trials and could, if injuries occur, result in product liability litigation. If serious adverse events or other undesirable side effects or unexpected characteristics of our gammaCore therapy or future product candidates are observed in investigator-sponsored trials, further clinical development of such product candidate may be delayed or we may not be able to continue development of such product candidate at all, and the occurrence of these events could have a material adverse effect on our business. Undesirable side effects caused by our gammaCore therapy or future product candidates could also result in the delay or denial of regulatory clearance or approval by the FDA or other regulatory authorities or in more restrictive labels than we desire.
Clinical trials are very expensive, time-consuming and difficult to design and implement and involve uncertain outcomes. Furthermore, results of earlier preclinical studies and clinical trials may not be predictive of results of future preclinical studies or clinical trials.
The risk of failure for our gammaCore therapy in additional treatment areas is high. It is difficult if not impossible to predict when or if any of our product candidates will receive regulatory clearance or approval in additional areas of indication outside of the acute treatment of eCH and the acute treatment of migraine. To obtain the requisite regulatory clearance or approvals to market and sell our gammaCore therapy in additional indications, we must demonstrate through extensive preclinical studies and clinical trials that it is safe and effective in humans for use in each additional target indication. Clinical testing is expensive and can take many years to complete, and the outcome is inherently uncertain. Failure can occur at any time during the clinical trial process.
In addition, the results of preclinical studies and early clinical trials may not be predictive of the results of later-stage preclinical studies or clinical trials. The results generated to date in preclinical studies or clinical trials for our gammaCore therapy in cluster and migraine headaches do not ensure that later preclinical studies or clinical trials will demonstrate similar results in other therapeutic indications, and it should be noted that we did not achieve the primary endpoints in our pivotal trials for cluster and migraine headaches. There can be no assurance that the FDA and other regulatory authorities will be satisfied by data from our clinical trials even where we believe such data to be compelling. Our gammaCore therapy may fail to show the desired safety and efficacy traits in additional areas of indication in future clinical trials despite having progressed through preclinical and earlier stage clinical trials. Many companies in the pharmaceutical and medical device industries have suffered significant setbacks in later-stage clinical trials due to lack of efficacy or adverse safety profiles, notwithstanding promising results in earlier trials, and we cannot be certain that we will not face similar setbacks. Moreover, preclinical and clinical data are often susceptible to varying interpretations and analyses, and many companies that have believed their product candidates performed satisfactorily in preclinical studies and clinical trials have nonetheless failed to obtain marketing clearance or approval of their products.
In some instances, there can be significant variability in safety or efficacy results between different clinical trials of the same product candidate due to numerous factors, including changes in clinical trial procedures set forth in protocols, differences in the size and type of the patient populations, adherence to the dosing regimen and other clinical trial protocols, and the rate of dropout among clinical trial participants. If we fail to produce positive results in our planned preclinical studies or clinical trials of any of our product candidates, the development timeline and regulatory approval and commercialization prospects for our product candidates, and, correspondingly, our business and financial prospects, would be materially adversely affected.
21
Table of Contents
We depend on enrollment of patients in our clinical trials for our product candidates. If we are unable to enroll patients in our clinical trials, our research and development efforts could be adversely affected.
Identifying and qualifying patients to participate in clinical trials for our gammaCore therapy in additional areas of indications is critical to our success. Successful and timely completion of clinical trials will require that we enroll a sufficient number of patients who remain in the study until its conclusion. If we are unable to enroll a sufficient number of patients in our clinical trials, our timelines for recruiting patients, conducting clinical trials and obtaining regulatory clearance or approval of our gammaCore therapy in additional areas of indication may be delayed. These delays could result in increased costs, delays in advancing our product development, delays in testing the effectiveness of our technology or termination of our clinical trials altogether.
We cannot predict how successful we will be at enrolling patients in future clinical trials. Patient enrollment is affected by other factors including:
| • | the eligibility criteria for the trial in question; |
| • | the perceived risks and benefits of the product candidate in the trial; |
| • | clinicians’ and patients’ perceptions as to the potential advantages of the product candidate being studied in relation to other available therapies, including any new drugs that may be approved for the indications we are investigating or drugs that may be used off-label for these indications; |
| • | the size of the patient population required for analysis of the trial’s primary endpoints; |
| • | competition for patients for competitive product candidates undergoing clinical trials; |
| • | the efforts to facilitate timely enrollment in clinical trials; |
| • | the design of the trial; |
| • | the patient referral practices of physicians; |
| • | our ability to recruit clinical trial investigators with the appropriate competencies and experience; |
| • | the ability to monitor patients adequately during and after treatment; |
| • | the risk that patients enrolled in clinical trials will drop out of the trials before completion; |
| • | the ability to obtain and maintain patient consents; |
| • | the number of patients with the indication being studied and the difficult of diagnosing the relevant condition or disease; and |
| • | the proximity and availability of clinical trial sites for prospective patients. |
In addition, our clinical trials will compete with other clinical trials that are in the same therapeutic areas as we are targeting, and this competition will reduce the number and types of patients available to us, because some patients who might have opted to enroll in our trials may instead opt to enroll in a trial being conducted by one of our competitors.
Delays in the completion of any clinical trial of our gammaCore therapy will increase our costs, slow down our expansion into additional treatment indications and approval process, and delay or potentially jeopardize our ability to commence product sales and generate future revenue. In addition, many of the factors that may lead to a delay in the commencement or completion of clinical trials may also ultimately lead to the denial of regulatory clearance or approval of our gammaCore therapy in additional treatment indications.
22
Table of Contents
Clinical trials may be delayed, suspended or terminated for many reasons, which will increase our expenses and delay the time it takes to develop and expand our gammaCore therapy in additional treatment indications.
We may experience delays in our ongoing or future preclinical studies or clinical trials, and we do not know whether future preclinical studies or clinical trials will begin on time, need to be redesigned, enroll an adequate number of patients on time or be completed on schedule, if at all. The commencement and completion of clinical trials for the expansion of our gammaCore therapy in additional areas of indication, such as Sjôgren’s syndrome and rheumatoid arthritis, may be delayed, suspended or terminated as a result of many factors, including:
| • | the FDA or other regulators disagreeing as to the design, protocol or implementation of our clinical trials; |
| • | the delay or refusal of regulators or institutional review boards, or IRBs, to authorize us to commence a clinical trial at a prospective trial site; |
| • | changes in regulatory requirements, policies and guidelines; |
| • | delays or failure to reach agreement on acceptable terms with prospective clinical research organizations, or CROs, and clinical trial sites, the terms of which can be subject to extensive negotiation and may vary significantly among different CROs and trial sites; |
| • | delays in patient enrollment and variability in the number and types of patients available for clinical trials; |
| • | the inability to enroll a sufficient number of patients in trials, particularly in orphan indications, to observe statistically significant treatment effects in the trial; |
| • | having clinical sites deviate from the trial protocol or dropping out of a trial; |
| • | negative or inconclusive results from ongoing preclinical studies or clinical trials, which may require us to conduct additional preclinical studies or clinical trials or to abandon projects that we expect to be promising; |
| • | safety or tolerability concerns that could cause us to suspend or terminate a trial if we find that the participants are being exposed to unacceptable health risks; |
| • | reports from preclinical or clinical testing of other similar therapies that raise safety or efficacy concerns; |
| • | regulators or IRBs requiring that we or our investigators suspend or terminate clinical research for various reasons, including noncompliance with regulatory requirements or safety concerns, among others; |
| • | lower than anticipated retention rates of patients and volunteers in clinical trials; |
| • | our CROs or clinical trial sites failing to comply with regulatory requirements or meet their contractual obligations to us in a timely manner, or at all, deviating from the protocol or dropping out of a trial; |
| • | delays relating to adding new clinical trial sites; |
| • | difficulty in maintaining contact with patients after treatment, resulting in incomplete data; |
| • | delays in establishing the appropriate dosage levels; |
| • | the quality of the product candidate falling below acceptable standards; |
| • | the inability to manufacture sufficient quantities of our gammaCore therapy to commence or complete clinical trials; and |
23
Table of Contents
| • | exceeding budgeted costs due to difficulty in accurately predicting costs associated with clinical trials. |
We could also encounter delays if a clinical trial is suspended or terminated by us, by the IRBs or Ethics Committees of the institutions at which such trials are being conducted, by the Data Safety Monitoring Board for such trial or by the FDA or other regulatory authorities. Such authorities may suspend or terminate a clinical trial due to a number of factors, including failure to conduct the clinical trial in accordance with regulatory requirements, including the FDA’s current Good Clinical Practice, or GCP, regulations, or our clinical protocols, inspection of the clinical trial operations or trial site by the FDA resulting in the imposition of a clinical hold, unforeseen safety issues or adverse side effects, failure to demonstrate a benefit from using a drug, changes in governmental regulations or administrative actions or lack of adequate funding to continue the clinical trial.
In addition, we may encounter delays if the FDA concludes that our financial relationships with investigators results in a perceived or actual conflict of interest that may have affected the interpretation of a study, the integrity of the data generated at the applicable clinical trial site or the utility of the clinical trial itself. Principal investigators for our clinical trials may serve as scientific advisors or consultants to us from time to time and receive cash compensation and/or stock options in connection with such services. If these relationships and any related compensation to or ownership interest by the clinical investigator carrying out the study result in perceived or actual conflicts of interest, or if the FDA concludes that the financial relationship may have affected interpretation of the study, the integrity of the data generated at the applicable clinical trial site may be questioned and the utility of the clinical trial itself may be jeopardized, which could result in the delay or rejection by the FDA. Any such delay or rejection could prevent us from commercializing any of our products currently in development.
If we experience delays in the commencement or completion of any clinical trial of our product candidates, or if any of our clinical trials are terminated, the commercial prospects of our gammaCore therapy may be harmed, and our ability to generate revenue from sales may be delayed or materially diminished.
We do not know whether any of our future preclinical studies or clinical trials will begin as planned, will need to be restructured or will be completed on schedule, or at all. Any delays in completing our clinical trials will increase our costs, slow down our product candidate development and approval process and jeopardize our ability to commence sales and generate associated revenue. Any of these occurrences may significantly harm our business, financial condition and prospects. In addition, many of the factors that cause, or lead to, a delay in the commencement or completion of clinical trials may also ultimately lead to the denial, suspension or revocation of expanded regulatory clearance or approval of our product candidates. Significant preclinical study or clinical trial delays also could shorten any periods during which we may have the exclusive right to commercialize our product candidates or allow our competitors to bring products to market before we do and impair our ability to successfully commercialize our product candidates.
Even if our products are approved or cleared in the United States and European Economic Area, or EEA, (which is composed of the 28 Member States of the EU plus Norway, Iceland and Liechtenstein), comparable regulatory authorities of additional foreign countries must also approve the manufacturing and marketing of our products in those countries. Approval and clearance procedures vary among jurisdictions and can involve requirements and administrative review periods different from, and greater than, those in the United States or the EEA, including additional preclinical studies or clinical trials. Any of these occurrences may harm our business, financial condition and prospects significantly.
If we fail to properly manage our anticipated growth, our business could suffer.
We have been growing rapidly in recent periods and have a relatively short history of operating as a commercial company. We intend to continue to grow and may experience periods of rapid growth and
24
Table of Contents
expansion, which could place a significant additional strain on our limited personnel, information technology systems and other resources. In particular, expanding our direct sales force in the United States requires significant management, financial and other supporting resources. Any failure by us to manage our growth effectively could have an adverse effect on our ability to achieve our development and commercialization goals.
To achieve our goals, we must successfully increase manufacturing output to meet potential expected customer demand. In the future, we may experience difficulties with manufacturing, quality control, component supply, inventory, distribution and shortages of qualified personnel, among other problems. These problems could result in delays in availability of our gammaCore therapy and increases in expenses. Any such delay or increased expense could adversely affect our ability to generate our revenue.
Future growth will also impose significant added responsibilities on management, including the need to identify, recruit, train and integrate additional employees. In addition, rapid and significant growth will place a strain on our administrative and operational infrastructure.
In order to manage our operations and growth we will need to continue to improve our operational and management controls, reporting and information technology systems and financial internal control procedures. If we are unable to manage our growth effectively, it may be difficult for us to execute our business strategy and our operating results and business could suffer.
If we fail to develop and retain an effective direct sales force in the United States, our business could suffer.
In order to commercialize our gammaCore therapy for the acute treatment of eCH and the acute treatment of migraine, in the United States, we must continue to build a substantial direct sales force. As we initiate our commercial launch in eCH and migraine and increase our marketing efforts, we will need to retain, grow and develop our direct sales personnel. We intend to make a significant investment in recruiting and training sales representatives and there is significant competition for such personnel. Once hired, the training process is lengthy because it requires significant education for new sales representatives to achieve the level of clinical competency with our products expected by physicians. Upon completion of the training, our sales representatives typically require lead time in the field to grow their network of accounts and achieve the productivity levels we expect them to reach in any individual territory. Furthermore, the use of our products often requires or benefits from direct support from us. If we are unable to attract, motivate, develop and retain a sufficient number of qualified sales personnel, and if our sales representatives do not achieve the productivity levels we expect them to reach, our revenue will not grow at the rate we expect and our financial performance will suffer. Also, to the extent we hire personnel from our competitors, we may have to wait until applicable non-competition provisions have expired before deploying such personnel in restricted territories or incur costs to relocate personnel outside of such territories, and we have been in the past, and may be subject to future allegations that these new hires have been improperly solicited, or that they have divulged to us proprietary or other confidential information of their former employers. Any of these risks may adversely affect our business.
We only recently began commercializing our gammaCore therapy for the acute treatment of eCH and acute treatment of migraine headache in the United States and we may never achieve market acceptance.
We have a limited history of commercializing our product outside the United States, and a very limited history of selling our gammaCore therapy in the United States. Our gammaCore therapy received de novo grant and clearance by the FDA for the acute treatment of pain associated with episodic CH in adults in April 2017. Additionally, our gammaCore therapy was cleared by the FDA in January 2018 for the acute treatment of pain associated with migraine in adults. Furthermore, our gammaCore therapy has not yet been cleared by the FDA for treatment of chronic cluster headache or preventive treatment of CH
25
Table of Contents
or migraine. We have limited experience engaging in commercial activities and limited established relationships with physicians, hospitals and payors as well as third-party suppliers on whom we depend for the manufacture of our product. We may be unable to gain broader market acceptance in the countries in which we have already begun to commercialize our gammaCore therapy, or, if approved by the FDA for additional indications, unable to successfully commercialize it in the United States for a number of reasons, including:
| • | established competitors with strong relationships with customers, including physicians, hospitals and third-party suppliers; |
| • | limitations in our ability to demonstrate differentiation and advantages of our product compared to competing products and the relative safety, efficacy and ease of use of our product; |
| • | the limited size of our sales force and the learning curve required to gain experience selling our product; |
| • | the inability to obtain sufficient supply of the components for our gammaCore therapy or secure second-source suppliers if our main suppliers are unable to fulfill our orders; |
| • | insufficient financial or other resources to support our commercialization efforts necessary to reach profitability; and |
| • | the introduction and market acceptance of new, more effective or less expensive competing products and technologies. |
If our competitors are better able to develop and market CH and migraine treatments that are safer, more effective, less costly, easier to use or otherwise more attractive than our gammaCore therapy, our business will be adversely impacted.
The pharmaceutical and medical device industries are highly competitive and subject to rapid innovation and change. Our success depends, in part, upon our ability to establish a competitive position in the cluster and migraine markets by securing broad market acceptance of our gammaCore therapy. We believe that the primary competitive factors in the cluster and migraine markets are demonstrated clinical effectiveness, product safety, reliability and durability, ease of use, product support and service, minimal side effects and salesforce experience and relationships. We face significant competition in the United States and internationally, which we believe will intensify over time. Many of the companies developing or marketing competing products enjoy several advantages over us, including:
| • | more experienced sales forces; |
| • | greater name recognition; |
| • | more established sales and marketing programs and distribution networks; |
| • | earlier regulatory clearance or approval; |
| • | long established relationships with physicians and hospitals; |
| • | significant patent portfolios, including issued U.S. and foreign patents and pending patent applications, as well as the resources to enforce patents against us or any of our third-party suppliers and distributors; |
| • | the ability to acquire and integrate our competitors and/or their technology; |
| • | demonstrated ability to develop product enhancements and new product offerings; |
| • | established history of product reliability, safety and durability; |
| • | the ability to offer rebates or bundle multiple product offerings to offer greater discounts or incentives; |
| • | greater financial and human resources for product development, sales, and marketing; and |
26
Table of Contents
| • | greater experience in and resources for conducting research and development, clinical studies, manufacturing, preparing regulatory submissions, obtaining regulatory clearance or approval for products and marketing approved products. |
Our competitors may develop and patent processes or products earlier than us, obtain patents that may apply to us at any time, obtain regulatory clearance or approvals for competing products or processes more rapidly than us or develop more effective or less expensive products or technologies that render our technology or products obsolete or less competitive. We also face fierce competition in recruiting and retaining qualified sales, scientific, and management personnel, establishing clinical trial sites and enrolling patients in clinical studies. If our competitors are more successful than us in these matters, our business may be harmed.
Many of our competitors are large, well-established companies with substantially greater resources than us and have a long history of competing in the CH and migraine markets.
Many of our current and potential competitors are publicly traded, or are divisions of publicly-traded, major pharmaceutical and medical device companies that have substantially greater financial, technical, sales and marketing resources than we do. We will face steep competition from Allergan, Amgen, Novartis and Teva, all of which are better capitalized and have a history of commercializing products around the world. We estimate the addressable U.S. market for eCH and migraine headache will be approximately $400 million and $3.8 billion in 2018, respectively. Given the size of the existing and potential market in the United States, we expect that as we continue and try to expand our commercial efforts in the United States our current and future competitors will take aggressive action to protect their current market position. We will face significant competition in establishing our market share in the United States and may encounter unforeseen obstacles and competitive challenges in the United States.
In addition, we face a particular challenge overcoming the long-standing practices by some physicians of using the headache products of our larger, more established competitors. Physicians who use our competitors’ products for the treatment of cluster and migraine headache may be reluctant to try new products from a source with which they are less familiar. If these physicians do not try and subsequently adopt our product, then our financial performance will be adversely affected.
Further, a number of our competitors are currently conducting, or we anticipate will be conducting, clinical trials to demonstrate the results of their headache products. The results of these trials may be equivalent to, or potentially better than, the results of our clinical trials, which could have a material adverse effect on us.
Traditional products used to treat CH and migraine have been available for decades, while our gammaCore therapy has only been commercially available in Europe for several years, and for less than one year in the United States, and, as a result, we have a limited track record compared to our competitors.
Traditional products used to treat CH and migraine have been commercially available for decades, while we only began commercializing our gammaCore therapy in Europe to treat CH and migraine several years ago, and within the past year in the United States. Because we have a limited commercial track record compared to our competitors and our gammaCore therapy generally has been utilized by patients for less time than other headache therapies, physicians may be slower to adopt or recommend our gammaCore therapy. Further, while we believe our international commercial experience and our clinical trials support the safety and effectiveness of our gammaCore therapy for the acute treatment of eCH and migraine headache, future studies or patient experience over a longer period of time may indicate that treatment with gammaCore is less attractive than treatment with competitive products or that our gammaCore therapy causes unexpected or serious complications or other unforeseen negative effects. Such results would likely slow the adoption of our gammaCore therapy and significantly reduce our sales, which would harm our business and adversely affect our results of operations. Furthermore, if patients with traditional or other headache products were to
27
Table of Contents
experience unexpected or serious complications or other unforeseen effects, the market for our gammaCore therapy may be adversely affected, even if such effects are not directly attributable to our gammaCore therapy.
We may expend our limited resources to pursue a particular product candidate or disease and fail to capitalize on product candidates or diseases that may be more profitable or for which there is a greater likelihood of success.
Because we have limited financial and managerial resources, we focus our research programs and product candidates on specific conditions. As a result, we may forego or delay pursuit of opportunities with other product candidates or other diseases or conditions that may later prove to have greater commercial potential. Our resource allocation decisions may cause us to fail to capitalize on viable commercial products or profitable market opportunities. Our spending on current and future research and development programs and product candidates for specific conditions may not yield any commercially viable products.
Our international operations subject us to certain operating risks, which could adversely impact our results of operations and financial condition.
Sales of gammaCore outside the United States represented a substantial portion of our net sales in the years ended December 31, 2016 and 2017, respectively. In 2012, we began selling gammaCore in the EU through distributors. As of February 1, 2018, we sell gammaCore directly in 14 countries in the EU and through distributors and agents located in Munich, Germany and Leeds, UK. The sale and shipment of gammaCore across international borders, as well as the purchase of components from international sources, subjects us to U.S. and foreign governmental trade, import and export, and customs regulations and laws.
Compliance with these regulations and laws is costly and exposes us to penalties for non-compliance. Other laws and regulations that can significantly impact us include various anti-bribery laws, including the U.S. Foreign Corrupt Practices Act, as well as export controls laws. Any failure to comply with applicable legal and regulatory obligations could impact us in a variety of ways that include, but are not limited to, significant criminal, civil and administrative penalties, including imprisonment of individuals, fines and penalties, denial of export privileges, seizure of shipments, restrictions on certain business activities and exclusion or debarment from government contracting.
Our international operations expose us and our distributors to risks inherent in operating in foreign jurisdictions. These risks include:
| • | difficulties in enforcing our intellectual property rights and in defending against third-party threats and intellectual property enforcement actions against us, our distributors or any of our third-party suppliers; |
| • | reduced or varied protection for intellectual property rights in some countries; |
| • | pricing pressure that we may experience internationally; |
| • | a shortage of high-quality salespeople and distributors; |
| • | third-party reimbursement policies that may require some of the patients who receive our products to directly absorb medical costs or that may necessitate the reduction of the selling prices of gammaCore; |
| • | competitive disadvantage to competition with established business and customer relationships; |
| • | foreign currency exchange rate fluctuations; |
| • | the imposition of additional U.S. and foreign governmental controls or regulations; |
| • | economic instability; |
28
Table of Contents
| • | changes in duties and tariffs, license obligations and other non-tariff barriers to trade; |
| • | the imposition of restrictions on the activities of foreign agents, representatives and distributors; |
| • | scrutiny of foreign tax authorities which could result in significant fines, penalties and additional taxes being imposed on us; |
| • | laws and business practices favoring local companies; |
| • | longer payment cycles; |
| • | difficulties in maintaining consistency with our internal guidelines; |
| • | difficulties in enforcing agreements and collecting receivables through certain foreign legal systems; |
| • | the imposition of costly and lengthy new export licensing requirements; |
| • | the imposition of U.S. or international sanctions against a country, company, person or entity with whom we do business that would restrict or prohibit continued business with the sanctioned country, company, person or entity; and |
| • | the imposition of new trade restrictions. |
If we experience any of these risks, our sales in non-U.S. jurisdictions may be harmed and our results of operations would suffer.
Our results may be impacted by changes in foreign currency exchange rates.
We have international operations and, as a result, an increase in the value of the U.S. dollar relative to foreign currencies could require us to reduce our selling price or risk making our products less competitive in international markets, or our costs could increase. Also, if our international sales increase, we may enter into a greater number of transactions denominated in non-U.S. dollars, which could expose us to increased foreign currency risks, including currency fluctuations and exchange rate risks. We do not currently engage in any hedging transactions. If we are unable to address these risks and challenges effectively, our international operations may not be successful and our business could be harmed.
We may not be able to establish or strengthen our brand.
We believe that establishing and strengthening the electroCore and gammaCore brands is critical to achieving widespread acceptance of our gammaCore therapy to treat eCH and migraine, particularly because of the highly competitive nature of the market for headache therapies. Promoting and positioning our brand will depend largely on the success of our marketing efforts and our ability to provide physicians with a reliable product for successful treatment of cluster and migraine headaches. Given the established nature of our competitors, and our lack of commercialization in the United States, it is likely that our future marketing efforts will require us to incur significant additional expenses. These brand promotion activities may not yield increased sales and, even if they do, any sales increases may not offset the expenses we incur to promote our brand. If we fail to successfully promote and maintain our brand, or if we incur substantial expenses in an unsuccessful attempt to promote and maintain our brand, our gammaCore therapy may not be accepted by physicians, which would adversely affect our business, results of operations and financial condition.
We may face product liability claims that could result in costly litigation and significant liabilities.
Manufacturing and marketing of gammaCore, and clinical testing of our gammaCore therapy to initially treat eCH and migraine, may expose us to individual product liability claims, class action lawsuits or actions, and other individual or mass tort claims. Although we have, and intend to maintain, liability
29
Table of Contents
insurance, the insurers may deny our claims, coverage limits of our insurance policies may not be adequate and one or more successful claims brought against us may have a material adverse effect on our business and results of operations. These risks are heightened in the event any product recalls take place as a result of any product design defect or defect in product warnings or labeling. Product liability claims could negatively affect our reputation, our continued product sales and our ability to obtain and maintain regulatory clearance or approval for our products.
If we fail to retain our key executives or recruit and hire new employees, our operations and financial results may be adversely effected while we attract other highly qualified personnel.
Our future success depends, in part, on our ability to continue to retain our executive officers and other key employees and recruit and hire new employees. All of our executive officers and other employees are at-will employees, and therefore may terminate employment with us at any time with no advance notice. The replacement of any of our key personnel likely would involve significant time and costs, may significantly delay or prevent the achievement of our business objectives and may harm our business.
In addition, many of our employees have become or will soon become vested in a substantial amount of stock or number of stock options. Our employees may be more likely to leave us if the shares they own or the shares underlying their vested options have significantly appreciated in value relative to the original purchase prices of the shares or the exercise prices of the options, or if the exercise prices of the options that they hold are significantly below the market price of our common stock. Further, our employees’ ability to exercise those options and sell their stock in a public market after the closing of this offering may result in a higher than normal turnover rate.
Our future success also depends on our ability to retain executive officers and other key employees and attract new key employees. Many executive officers and employees in the pharmaceutical and medical device industries are subject to strict non-compete or confidentiality agreements with their employers, which may include our main competitors. In addition, some of our existing and future employees are or may be subject to confidentiality agreements with previous employers. Our competitors may allege breaches of and seek to enforce such non-compete agreements or initiate litigation based on such confidentiality agreements. Such litigation, whether or not meritorious, may impede our ability to attract or use executive officers and other key employees who have been employed by our competitors and may result in intellectual property claims against us. It is likely that we will experience similar aggressive lawsuit tactics by our competitors as they seek to protect their market position, particularly as we prepare to expand in new or existing markets.
Our employees, independent contractors, consultants, commercial collaborators, principal investigators, CROs and vendors may engage in misconduct or other improper activities, including non-compliance with regulatory standards and requirements.
We are exposed to the risk that our employees, independent contractors, consultants, commercial collaborators, principal investigators, CROs and vendors may engage in fraudulent conduct or other illegal activity. Misconduct by these parties could include intentional, reckless or negligent conduct or unauthorized activities that violates (1) the laws and regulations of the FDA and other similar regulatory authorities, including those laws requiring the reporting of true, complete and accurate information to such authorities, (2) manufacturing standards, (3) federal and state data privacy, security, fraud and abuse and other healthcare laws and regulations in the United States and abroad and (4) laws that require the true, complete and accurate reporting of financial information or data. In particular, sales, marketing and business arrangements in the healthcare industry are subject to extensive laws and regulations intended to prevent fraud, misconduct, kickbacks, self-dealing and other abusive practices. These laws and regulations may restrict or prohibit a wide range of pricing, discounting, marketing and promotion, sales commission, customer incentive programs and other business arrangements. Misconduct by these parties could also involve the improper use of individually identifiable information,
30
Table of Contents
including information obtained in the course of clinical trials, creating fraudulent data in our preclinical studies or clinical trials or illegal misappropriation of product candidates, which could result in regulatory sanctions and serious harm to our reputation.
Although we intend to adopt a code of business conduct and ethics, it is not always possible to identify and deter misconduct by employees and other third parties, and the precautions we take to detect and prevent this activity may not be effective in controlling unknown or unmanaged risks or losses or in protecting us from governmental investigations or other actions or lawsuits stemming from a failure to be in compliance with such laws or regulations. Additionally, we are subject to the risk that a person or government could allege such fraud or other misconduct, even if none occurred. If any such actions are instituted against us, and we are not successful in defending ourselves or asserting our rights, those actions could have a significant impact on our business, including the imposition of significant civil, criminal and administrative penalties, including damages, fines, disgorgement, imprisonment, exclusion from participation in government healthcare programs, such as Medicare and Medicaid, contractual damages, reputational harm and the curtailment or restructuring of our operations.
Risk Related to our Dependence on Third Parties
We rely upon third-party, single-source, and in certain cases sole-source, suppliers for many of the components and materials used in gammaCore, and for critical manufacturing and packaging services, making us vulnerable to supply shortages and problems and price fluctuations, which could harm our business.
A number of the critical components used in gammaCore are supplied to us from single-source, or in certain cases sole-source, suppliers. Our suppliers may encounter problems during manufacturing for a variety of reasons, including, for example, failure to follow specific protocols and procedures, failure to comply with applicable legal and regulatory requirements, equipment malfunction and environmental factors, failure to properly conduct their own business affairs, and infringement of third-party intellectual property rights, any of which could delay or impede their ability to meet our requirements. Our ability to supply gammaCore commercially depends, in part, on our ability to obtain a supply of these components that has been manufactured in accordance with regulatory requirements and in sufficient quantities for commercialization and clinical testing. We have not entered into manufacturing, supply or quality agreements with all of our single-source and sole-source suppliers, some of which supply components critical to our products. We are not certain that our single-source or sole-source suppliers will be able to meet our demand for their products and services, either because of the nature of our agreements with those suppliers, or our limited experience with those suppliers, or due to our relative importance as a customer to those suppliers. It may be difficult for us to assess their ability to timely meet our demand in the future based on past performance. While our suppliers have generally met our demand for their products on a timely basis in the past, they may subordinate our needs in the future to their other customers.
Establishing additional or replacement suppliers for the components or processes used in gammaCore, if required, may not be accomplished quickly. If we are able to find a replacement supplier, such replacement supplier would need to be qualified and may require additional regulatory authority approval, which could result in further delay. While we seek to maintain adequate inventory of the single-source or sole-source components and materials used in our products, any interruption or delay in the supply of components or materials, or our inability to obtain components or materials from alternate sources at acceptable prices in a timely manner, could impair our ability to meet the demand of our customers and cause them to cancel orders.
If our third-party suppliers fail to deliver the required commercial quantities of materials, or the level of services we require, on a timely basis and at commercially reasonable prices, and we are unable to find one or more replacement suppliers capable of production at a substantially equivalent cost in substantially equivalent volumes and quality and on a timely basis, the continued commercialization of
31
Table of Contents
gammaCore would be impeded, delayed, limited or prevented, which could harm our business, results of operations, financial condition and prospects.
We rely in part on a small group of third-party distributors to effectively distribute our products outside the United States.
We depend in part on a small group of third-party distributors for the marketing and selling of our products in certain territories in Europe. We depend on these distributors’ efforts to market our products, yet we are unable to control their efforts completely. These distributors typically sell a variety of other non-competing products that may limit the resources they dedicate to selling our gammaCore therapy. In addition, we are unable to ensure that our distributors comply with all applicable laws regarding the sale of our products. If our distributors fail to effectively market and sell gammaCore in full compliance with applicable laws, our operating results and business may suffer. Recruiting and retaining qualified third-party distributors and training them in our technology and product offerings requires significant time and resources. To develop and expand our distribution, we must continue to scale and improve our processes and procedures that support our distributors. Further, if our relationship with a successful distributor terminates, we may be unable to replace that distributor without disruption to our business. If we fail to maintain positive relationships with our distributors, fail to develop new relationships with other distributors, including in new markets, fail to manage, train or incentivize existing distributors effectively, or fail to provide distributors with competitive products on attractive terms, or if these distributors are not successful in their sales efforts, our revenue may decrease and our operating results, reputation and business may be harmed.
We intend to rely upon only one third-party distributor to distribute our products in the United States.
We intend to rely upon one specialty pharmaceutical distributor, comprised of a large network of specialty pharmacies, to distribute our products in the United States. We depend on this distributor to distribute our products, but are unable to control its performance. This distributor may distribute a variety of other specialty pharmaceutical products that may limit the resources dedicated to the distribution of our products. In addition, we are unable to ensure that this distributor will comply with all applicable laws related to the distribution of our products. If this distributor fails to distribute our products in compliance with applicable laws, our operating results and business may suffer. Recruiting, training and retaining third-party distributors in the distribution of our proprietary product offerings requires significant time and resources. In addition, an affiliate of this distributor provides pharmaceutical patient hub services for patients that are prescribed our gammaCore therapy, and has been electronically integrated with our proprietary data warehouse system and web portal. If our relationship with this distributor terminates, we may be unable to replace this distributor without disruption to our business. Any new distributor may not integrate as seamlessly with our data warehouse system and web portal, leading to disruptions in service for patients that are prescribed our therapy, which may cause these patients to seek alternative therapy. Our distributor also may not pay us on time or at all due to disputes, financial issues or bankruptcy events. Any such payment issues may materially affect our operating results until we are able to resolve the issues, or find a sufficient replacement for our distributor.
We rely on third parties to conduct and support our clinical trials, and those third parties may not perform satisfactorily, including failing to meet deadlines for the completion of such trials.
We do not independently conduct clinical trials for our product candidates. We rely on third parties, such as CROs, clinical data management organizations, medical institutions and clinical investigators, to perform this function. Our reliance on these third parties for clinical development activities reduces our control over these activities but does not relieve us of our responsibilities. Furthermore, some of the sites for our clinical trials are outside the United States. The performance of these sites may be adversely affected by various issues, including less advanced medical infrastructure, lack of familiarity with
32
Table of Contents
conducting clinical trials in accordance with U.S. standards, insufficient training of personnel, communication difficulties or change in local regulations. We remain responsible for ensuring that each of our clinical trials is conducted in accordance with the general investigational plan and protocols for the study. Moreover, the FDA requires us to comply with GCP for conducting, recording and reporting the results of clinical trials to assure that data and reported results are credible and accurate and that the rights, integrity and confidentiality of patients in clinical trials are protected. Furthermore, these third parties may also have relationships with other entities, including our competitors. If these third parties do not successfully carry out their contractual duties, meet expected deadlines or conduct our clinical trials in accordance with regulatory requirements or our stated protocols, we will not be able to obtain, or may be delayed in obtaining, regulatory clearance or approval for our product candidates and will not be able to, or may be delayed in our efforts to, successfully commercialize our products.
We also rely on other third parties to store and distribute supplies for our clinical trials. Any performance failure on the part of our existing or future distributors could delay clinical development or regulatory clearance or approval of our product candidates or commercialization of our products, producing additional losses and depriving us of potential product revenues.
If we do not successfully enter into future collaborations for the development and commercialization of our gammaCore therapy in international markets our business may be harmed.
We may choose to enter into collaboration agreements with third parties with respect to development and commercialization of our gammaCore therapy in international markets. We will have limited control over the amount and timing of resources that our collaborators dedicate to the development or commercialization of our gammaCore therapy. Our ability to generate revenues from these arrangements will depend in part on our collaborators’ abilities to successfully perform the functions assigned to them in these arrangements.
Collaborations involving our gammaCore therapy, such as our collaboration with Desitin, are subject to numerous risks, which may include the following:
| • | collaborators have significant discretion in determining the efforts and resources that they will apply to a collaborations; |
| • | collaborators may not pursue development and commercialization of our product candidates or may elect not to continue or renew development or commercialization programs based on clinical trial results, changes in their strategic focus due to the acquisition of competitive products, availability of funding or other external factors, such as a business combination that diverts resources or creates competing priorities; |
| • | collaborators may delay clinical trials, provide insufficient funding for a clinical trial, stop a clinical trial, abandon a product candidate, repeat or conduct new clinical trials or require a new formulation of a product candidate for clinical testing; |
| • | collaborators could independently develop, or develop with third parties, products that compete directly or indirectly with our products or product candidates; |
| • | a collaborator with marketing and distribution rights to one or more products may not commit sufficient resources to their marketing and distribution; |
| • | collaborators may not properly maintain or defend our intellectual property rights or may use our intellectual property or proprietary information in a way that gives rise to actual or threatened litigation that could jeopardize or invalidate our intellectual property or proprietary information or expose us to potential liability; |
| • | disputes may arise between us and a collaborator that cause the delay or termination of the research, development or commercialization of our product candidates or that result in costly litigation or arbitration that diverts management attention and resources; |
33
Table of Contents
| • | collaborations may be terminated and, if terminated, may result in a need for additional capital to pursue further development or commercialization of the applicable product candidates; and |
| • | collaborators may own or co-own intellectual property covering our products that result from our collaborating with them, and in such cases, we would not have the exclusive right to commercialize such intellectual property. |
Any termination or disruption of any future collaboration could result in delayed development of product candidates, increased cost to develop product candidates or termination of development of a product candidate.
If we are not able to establish or maintain collaborations, we may have to alter some of our future development and commercialization plans.
Our product development programs and the potential commercialization of our gammaCore therapy will require substantial additional capital to fund expenses. For some of our product candidates, we may decide to collaborate with pharmaceutical and medical device companies for the future development and potential commercialization of those product candidates. Furthermore, we may find that our programs require the use of proprietary rights held by third parties, and the growth of our business may depend in part on our ability to acquire, in-license or use these proprietary rights.
We face significant competition in seeking appropriate collaborators, and a number of more established companies may also be pursuing strategies to license or acquire third-party intellectual property rights that we may consider attractive. These established companies may have a competitive advantage over us due to their size, financial resources and greater clinical development and commercialization capabilities. In addition, companies that perceive us to be a competitor may be unwilling to assign or license rights to us. Whether we reach a definitive agreement for a collaboration will depend upon, among other things, our assessment of the collaborator’s resources and expertise, the terms and conditions of the proposed collaboration and the proposed collaborator’s evaluation of a number of factors. Those factors may include the design or results of clinical trials, the likelihood of clearance or approval by the FDA, compliance with the Essential Requirements of the EU Medical Devices Directive or similar foreign regulations, the potential market for the subject product candidate, the costs and complexities of manufacturing and delivering such product candidate to patients, competing products, the existence of uncertainty with respect to our ownership of technology, which can exist if there is a challenge to such ownership without regard to the merits of the challenge, and industry and market conditions generally. The collaborator may also consider alternative product candidates or technologies for similar indications that may be available to collaborate on and whether such a collaboration could be more attractive than the one with us for our product candidate. We may also be restricted under existing license agreements from entering into agreements on certain terms with potential collaborators. Collaborations are complex and time-consuming to negotiate and document. In addition, there have been a significant number of recent business combinations among large pharmaceutical companies that have resulted in a reduced number of potential future collaborators. We may not be able to negotiate collaborations on a timely basis, on acceptable terms, or at all. Even if we are able to obtain a license to intellectual property of interest, we may not be able to secure exclusive rights, in which case others could use the same rights and compete with us. If we are unable to successfully obtain rights to required third-party intellectual property rights or maintain the existing intellectual property rights we have, we may have to curtail the development of such product candidate, reduce or delay its development program or one or more of our other development programs, delay its potential commercialization or reduce the scope of any sales or marketing activities, or increase our expenditures and undertake development or commercialization activities at our own expense. If we elect to increase our expenditures to fund development or commercialization activities on our own, we may need to obtain additional capital, which may not be available to us on acceptable terms, or at all. If we do not have sufficient funds, we may not be able to further develop our product candidates or bring them to market and generate product revenue.
34
Table of Contents
We, or third-party manufacturers on whom we rely, may be unable to successfully scale-up manufacturing of our gammaCore therapy or its component parts in sufficient quality and quantity, which would delay or prevent us from developing and commercializing any approved products.
In order to conduct clinical trials of our gammaCore therapy and commercialize any approved products, we, or our manufacturers, will need to manufacture them in large quantities. We, or our manufacturers, may be unable to successfully increase manufacturing capacity in a timely or cost-effective manner, or at all. In addition, quality issues may arise during scale-up activities. If we, or any of our manufacturers, are unable to successfully scale up manufacturing in sufficient quality and quantity, the development, testing, and clinical trials of our gammaCore therapy may be delayed or infeasible, and regulatory clearance, approval or commercial launch of any resulting product may be delayed or not obtained, which could significantly harm our business. If we are unable to obtain or maintain third-party manufacturing for commercial supply of our product candidates, or to do so on commercially reasonable terms, we may not be able to develop and commercialize our gammaCore therapy successfully.
We are required to maintain high levels of inventory due to our single-source supply vendors, which could consume a significant amount of our resources, reduce our cash flows and lead to inventory impairment charges.
Our gammaCore therapy consists of a substantial number of individual components. In order to market and sell gammaCore effectively, we often must maintain high levels of inventory of the product and its components. The manufacturing process requires lengthy lead times during which components of our gammaCore therapy may become obsolete, and we may over- or under-estimate the amount needed of a given component, in which case we may expend extra resources or be constrained in the amount of end product that we can produce. As compared to direct manufacturers, our dependence on third-party manufacturers exposes us to greater lead times increasing our risk of inventory obsolesce comparatively.
Risks Related to Intellectual Property
We rely on a variety of intellectual property rights, and if we are unable to maintain or protect our intellectual property, our business and results of operations will be harmed.
Our commercial success will depend, in part, on our ability to obtain and maintain intellectual property protection for our products, processes, and related technologies in the United States, Europe and elsewhere, successfully defend our intellectual property rights against third-party challenges and successfully enforce our intellectual property rights to prevent third-party infringement. While we rely primarily upon a combination of patents, copyrights, trademarks and trade secret protection, as well as nondisclosure, confidentiality and other contractual agreements to protect the intellectual property related to our brands, products and other proprietary technologies, protection derived from patents is relatively limited.
The process of obtaining patent protection is expensive and time-consuming, and we may not be able to prosecute all necessary or desirable patent applications at a reasonable cost or in a timely manner. We may choose not to seek patent protection for certain innovations or products and may choose not to pursue patent protection in certain jurisdictions, and under the laws of certain jurisdictions, patents or other intellectual property rights may be unavailable or limited in scope and, in any event, any patent protection we obtain may be limited. As a result, some of our products are not, and in the future may not be, protected by patents. We generally apply for patents in those countries where we intend to make, have made, use, offer for sale, or sell products and where we assess the risk of infringement to justify the cost of seeking patent protection. However, we do not seek protection in all countries where we sell products and we may not accurately predict all the countries where patent protection would ultimately be desirable. If we fail to timely file a patent application in any such country or major market, we may be precluded from doing so at a later date. Competitors may use our technologies in jurisdictions where we have not obtained patent protection to develop their own products and, further, may export otherwise
35
Table of Contents
infringing products to territories in which we have patent protection that may not be sufficient to terminate infringing activities.
Furthermore, we cannot guarantee that any patents will be issued from any pending or future owned or licensed patent applications, or that any current or future patents will provide us with any meaningful protection or competitive advantage. Even if issued, existing or future patents may be challenged, including with respect to ownership, narrowed, invalidated, held unenforceable or circumvented, any of which could limit our ability to prevent competitors and other third parties from developing and marketing similar products or limit the length of terms of patent protection we may have for our products and technologies. Other companies may also design around technologies we have patented, licensed or developed. In addition, the issuance of a patent does not give us the right to practice the patented invention. Third parties may have blocking patents that could prevent us from marketing our products or practicing our own patented technology.
The patent positions of pharmaceutical and medical device companies can be highly uncertain and involve complex legal, scientific and factual questions for which important legal principles remain unresolved. The standards that the USPTO and its foreign counterparts use to grant patents are not always applied predictably or uniformly. Changes in either the patent laws, implementing regulations or the interpretation of patent laws may diminish the value of our rights. The legal systems of certain countries do not protect intellectual property rights to the same extent as the laws of the United States, and many companies have encountered significant problems in protecting and defending such rights in foreign jurisdictions.
Because patent applications in the United States, Europe and many other jurisdictions are typically not published until 18 months after filing, or in some cases not at all, and because publications of discoveries in scientific literature lag behind actual discoveries, we cannot be certain that we were the first to conceive or reduce to practice the inventions claimed in our issued patents or pending patent applications, or that we were the first to file for protection of the inventions set forth in our patents or pending patent applications. We can give no assurance that all of the potentially relevant art relating to our patents and patent applications has been found; overlooked prior art could be used by a third party to challenge the validity, enforceability and scope of our patents or prevent a patent from issuing from a pending patent application. As a result, we may not be able to obtain or maintain protection for certain inventions. Therefore, the validity, enforceability and scope of our patents in the United States, Europe and in other countries cannot be predicted with certainty and, as a result, any patents that we own or license may not provide sufficient protection against our competitors.
Third parties may challenge any existing patent or future patent we own or license through adversarial proceedings in the issuing offices or in court proceedings, including as a response to any assertion of our patents against them. In any of these proceedings, a court or agency with jurisdiction may find our patents invalid and/or unenforceable, or even if valid and enforceable, insufficient to provide protection against competing products and services sufficient to achieve our business objectives. We may be subject to a third-party pre-issuance submission of prior art to the USPTO, or reexamination by the USPTO if a third party asserts a substantial question of patentability against any claim of a U.S. patent we own or license. The adoption of the Leahy-Smith America Invents Act, or the Leahy-Smith Act, in September 2011 established additional opportunities for third parties to invalidate U.S. patent claims, including inter partes review and post-grant review proceedings. Outside of the United States, patents we own or license may become subject to patent opposition or similar proceedings, which may result in loss of scope of some claims or the entire patent. In addition, such proceedings are very complex and expensive, and may divert our management’s attention from our core business. If any of our patents are challenged, invalidated, circumvented by third parties or otherwise limited or expire prior to the commercialization of our products, and if we do not own or have exclusive rights to other enforceable patents protecting our products or other technologies, competitors and other third parties could market products and use processes that are substantially similar to, or superior to, ours and our business would suffer.
36
Table of Contents
The degree of future protection for our proprietary rights is uncertain because legal means afford only limited protection and may not adequately protect our rights or permit us to gain or keep a competitive advantage. For example:
| • | others may be able to develop products that are similar to, or better than, ours in a way that is not covered by the claims of our patents; |
| • | we might not have been the first to conceive or reduce to practice the inventions covered by our patents or pending patent applications; |
| • | we might not have been the first to file patent applications for our inventions; |
| • | any patents that we obtain may not provide us with any competitive advantages or may ultimately be found invalid or unenforceable; or |
| • | we may not develop additional proprietary technologies that are patentable. |
We may become involved in lawsuits to protect or enforce our patents, which could be expensive, time-consuming and unsuccessful.
Competitors may infringe our patents. To counter infringement or unauthorized use, we may be required to file one or more lawsuit and assert infringement claims, which can be expensive and time-consuming. In addition, in an infringement proceeding, a court may decide that a patent of ours is invalid or unenforceable, or may refuse to enjoin the other party from using the technology at issue on the grounds that our patents do not cover the technology in question. The standards that courts use to interpret patents are not always applied predictably or uniformly and can change, particularly as new technologies develop. As a result, we cannot predict with certainty how much protection, if any, will be given to our patents if we attempt to enforce them and they are challenged in court. Further, even if we prevail against an infringer in U.S. district court, there is always the risk that the infringer will file an appeal and the district court judgment will be overturned at the appeals court and/or that an adverse decision will be issued by the appeals court relating to the validity or enforceability of our patents. An adverse result in any litigation proceeding could put one or more of our patents at risk of being invalidated or interpreted in a manner insufficient to achieve our business objectives.
Our commercial success depends significantly on our ability to operate without infringing upon the intellectual property rights of third parties.
The pharmaceutical and medical device industries are subject to rapid technological change and substantial litigation regarding patent and other intellectual property rights. Our competitors in both the United States and abroad, many of which have substantially greater resources and have made substantial investments in patent portfolios and competing technologies, may have applied for or obtained or may in the future apply for or obtain, patents that will prevent, limit or otherwise interfere with our ability to make, use and sell our products and services. Numerous third-party patents exist in the fields relating to our products and services, and it is difficult for industry participants, including us, to identify all third-party patent rights relevant to our products, services and technologies. Moreover, because some patent applications are maintained as confidential for a certain period of time, we cannot be certain that third parties have not filed patent applications that cover our products, services and technologies.
Patents could be issued to third parties that we may ultimately be found to infringe. Third parties may have or obtain valid and enforceable patents or proprietary rights that could block us from developing products using our technology. Our failure to obtain or maintain a license to any technology that we require may materially harm our business, financial condition and results of operations. Furthermore, we would be exposed to a threat of litigation.
From time to time, we may be party to, or threatened with, litigation or other proceedings with third parties, including non-practicing entities, who allege that our products, components of our products,
37
Table of Contents
services, and/or proprietary technologies infringe, misappropriate or otherwise violate their intellectual property rights. The types of situations in which we may become a party to such litigation or proceedings include:
| • | we or our collaborators may initiate litigation or other proceedings against third parties seeking to invalidate the patents held by those third parties or to obtain a judgment that our products or processes do not infringe those third parties’ patents; |
| • | we or our collaborators may participate at substantial cost in International Trade Commission proceedings to abate importation of products that would compete unfairly with our products; |
| • | if our competitors file patent applications that claim technology also claimed by us or our licensors, we or our licensors may be required to participate in interference, derivation or opposition proceedings to determine the priority of invention, which could jeopardize our patent rights and potentially provide a third party with a dominant patent position; |
| • | if third parties initiate litigation claiming that our processes or products infringe their patent or other intellectual property rights, we and our collaborators will need to defend against such proceedings; |
| • | if third parties initiate litigation or other proceedings seeking to invalidate patents owned by or licensed to us or to obtain a declaratory judgment that their products, services, or technologies do not infringe our patents or patents licensed to us, we will need to defend against such proceedings; |
| • | we may be subject to ownership disputes relating to intellectual property, including disputes arising from conflicting obligations of consultants or others who are involved in developing our products; and |
| • | if a license to necessary technology is terminated, the licensor may initiate litigation claiming that our processes or products infringe or misappropriate its patent or other intellectual property rights and/or that we breached our obligations under the license agreement, and we and our collaborators would need to defend against such proceedings. |
These lawsuits and proceedings, regardless of merit, are time-consuming and expensive to initiate, maintain, defend or settle, and could divert the time and attention of managerial and technical personnel, which could materially adversely affect our business. Any such claim could also force use to do one or more of the following:
| • | incur substantial monetary liability for infringement or other violations of intellectual property rights, which we may have to pay if a court decides that the product, service, or technology at issue infringes or violates the third party’s rights, and if the court finds that the infringement was willful, we could be ordered to pay treble damages and the third party’s attorneys’ fees; |
| • | pay substantial damages to our customers or end users to discontinue use or replace infringing technology with non-infringing technology; |
| • | stop manufacturing, offering for sale, selling, using, importing, exporting or licensing the product or technology incorporating the allegedly infringing technology or stop incorporating the allegedly infringing technology into such product, service, or technology; |
| • | obtain from the owner of the infringed intellectual property right a license, which may require us to pay substantial upfront fees or royalties to sell or use the relevant technology and which may not be available on commercially reasonable terms, or at all; |
38
Table of Contents
| • | redesign our products, services, and technology so they do not infringe or violate the third party’s intellectual property rights, which may not be possible or may require substantial monetary expenditures and time; |
| • | enter into cross-licenses with our competitors, which could weaken our overall intellectual property position; |
| • | lose the opportunity to license our technology to others or to collect royalty payments based upon successful protection and assertion of our intellectual property against others; |
| • | find alternative suppliers for non-infringing products and technologies, which could be costly and create significant delay; or |
| • | relinquish rights associated with one or more of our patent claims, if our claims are held invalid or otherwise unenforceable. |
Some of our competitors may be able to sustain the costs of complex intellectual property litigation more effectively than we can because they have substantially greater resources. In addition, intellectual property litigation, regardless of its outcome, may cause negative publicity, adversely impact prospective customers, cause product shipment delays, or prohibit us from manufacturing, marketing or otherwise commercializing our products, services and technology. Any uncertainties resulting from the initiation and continuation of any litigation could have a material adverse effect on our ability to raise additional funds or otherwise have a material adverse effect on our business, results of operation, financial condition or cash flows.
In addition, we may indemnify our customers and distributors against claims relating to the infringement of intellectual property rights of third parties related to our products. Third parties may assert infringement claims against our customers or distributors. These claims may require us to initiate or defend protracted and costly litigation on behalf of our customers or distributors, regardless of the merits of these claims. If any of these claims succeed, we may be forced to pay damages on behalf of our customers, suppliers or distributors, or may be required to obtain licenses for the products or services they use. If we cannot obtain all necessary licenses on commercially reasonable terms, our customers may be forced to stop using our products or services.
Furthermore, because of the substantial amount of discovery required in connection with intellectual property litigation, there is a risk that some of our confidential information could be compromised by disclosure during this type of litigation. There could also be public announcements of the results of hearings, motions or other interim proceedings or developments, which could have a material adverse effect on the price of our common stock. If securities analysts or investors perceive these results to be negative, it could have a material adverse effect on the price of our common stock. The occurrence of any of these events may have a material adverse effect on our business, results of operation, financial condition or cash flows.
If we are unable to protect the confidentiality of our trade secrets, our business and competitive position may be harmed.
In addition to patent, copyright, and trademark protection, we also rely on trade secrets, including unpatented know-how, technology and other proprietary information, to maintain our competitive position. We seek to protect our trade secrets, in part, by entering into non-disclosure and confidentiality agreements with parties who have access to them, such as our consultants and vendors, or our former or current employees. We also enter into confidentiality and invention and patent assignment agreements with our employees and consultants. Despite these efforts, however, any of these parties may breach the agreements and disclose our trade secrets and other unpatented or unregistered proprietary information, and once disclosed, we are likely to lose trade secret protection. Monitoring unauthorized uses and
39
Table of Contents
disclosures of our intellectual property is difficult, and we do not know whether the steps we have taken to protect our intellectual property will be effective. In addition, we may not be able to obtain adequate remedies for any such breaches. Enforcing a claim that a party illegally disclosed or misappropriated a trade secret is difficult, expensive and time-consuming, and the outcome is unpredictable. In addition, some courts inside and outside the United States are less willing or unwilling to enforce trade secret protection.
Further, our competitors may independently develop knowledge, methods and know-how similar, equivalent, or superior to our proprietary technology. Competitors could purchase our products and attempt to reverse engineer and replicate some or all of the competitive advantages we derive from our development efforts, willfully infringe our intellectual property rights, design around our protected technology, or develop their own competitive technologies that fall outside of our intellectual property rights. In addition, our key employees, consultants, suppliers or other individuals with access to our proprietary technology and know-how may incorporate that technology and know-how into projects and inventions developed independently or with third parties. As a result, disputes may arise regarding the ownership of the proprietary rights to such technology or know-how, and any such dispute may not be resolved in our favor. If any of our trade secrets were to be lawfully obtained or independently developed by a competitor, we would have no right to prevent them, or those to whom they communicate it, from using that technology or information to compete with us and our competitive position could be adversely affected. If our intellectual property is not adequately protected so as to protect our market against competitors’ products and processes, our competitive position could be adversely affected, as could our business.
Changes in patent law could diminish the value of patents in general, thereby impairing our ability to protect our existing and future products and processes.
As is the case with other pharmaceutical and medical device companies, our success is heavily dependent on intellectual property, particularly patents. Obtaining and enforcing patents in the biopharmaceutical industry involves both technological and legal complexity, and is therefore costly, time-consuming, and inherently uncertain. In addition, the United States has recently enacted and is currently implementing wide-ranging patent reform legislation. Recent patent reform legislation could increase the uncertainties and costs surrounding the prosecution of our patent applications and the enforcement or defense of our issued patents. On September 16, 2011, the Leahy-Smith Act was signed into law. The Leahy-Smith Act includes a number of significant changes to U.S. patent law. These include provisions that affect the way patent applications are prosecuted, redefine prior art, may affect patent litigation, and switched the United States patent system from a “first-to-invent” system to a “first-to-file” system. Under a “first-to-file” system, assuming the other requirements for patentability are met, the first inventor to file a patent application generally will be entitled to the patent on an invention regardless of whether another inventor had conceived or reduced to practice the invention earlier. The USPTO recently developed new regulations and procedures to govern administration of the Leahy-Smith Act, and many of the substantive changes to patent law associated with the Leahy-Smith Act, in particular, the first-to-file provisions, only became effective on March 16, 2013. Accordingly, it is not clear what, if any, impact the Leahy-Smith Act will have on the operation of our business. The Leahy-Smith Act and its implementation could increase the uncertainties and costs surrounding the prosecution of our patent applications and the enforcement or defense of our issued patents, all of which could have a material adverse effect on our business and financial condition.
In addition, patent reform legislation may pass in the future that could lead to additional uncertainties and increased costs surrounding the prosecution, enforcement and defense of our patents and pending patent applications. Recent U.S. Supreme Court rulings have narrowed the scope of patent protection available in certain circumstances and weakened the rights of patent owners in certain situations. Furthermore, the U.S. Supreme Court and the U.S. Court of Appeals for the Federal Circuit have made,
40
Table of Contents
and will likely continue to make, changes in how the patent laws of the United States are interpreted. Similarly, foreign courts have made, and will likely continue to make, changes in how the patent laws in their respective jurisdictions are interpreted. We cannot predict future changes in the interpretation of patent laws or changes to patent laws that might be enacted into law by United States and foreign legislative bodies. Those changes may materially affect our patents or patent applications and our ability to obtain additional patent protection in the future.
Obtaining and maintaining patent protection depends on compliance with various procedural, document submission, fee payment and other requirements imposed by governmental patent agencies, and our patent protection could be reduced or eliminated for non-compliance with these requirements.
The USPTO and various foreign governmental patent agencies require compliance with a number of procedural, documentary, fee payment, and other similar provisions during the patent application process. In addition, periodic maintenance fees on issued patents often must be paid to the USPTO and foreign patent agencies over the lifetime of the patent. While an unintentional lapse can in many cases be cured by payment of a late fee or by other means in accordance with the applicable rules, there are situations in which noncompliance can result in abandonment or lapse of the patent or patent application, resulting in partial or complete loss of patent rights in the relevant jurisdiction. Non-compliance events that could result in abandonment or lapse of a patent or patent application include, but are not limited to, failure to respond to official actions within prescribed time limits, non-payment of fees and failure to properly legalize and submit formal documents. If we fail to maintain the patents and patent applications covering our products or procedures, we may not be able to stop a competitor from marketing products that are the same as or similar to our own, which would have a material adverse effect on our business.
If our trademarks and trade names are not adequately protected, then we may not be able to build name recognition in our markets of interest and our business may be adversely affected.
Our registered or unregistered trademarks or trade names may be challenged, infringed, circumvented, declared generic or determined to be infringing on other marks. We may not be able to protect our rights in these trademarks and trade names, which we need in order to build name recognition with potential partners or customers in our markets of interest. In addition, third parties have used trademarks similar and identical to our trademarks in foreign jurisdictions, and have filed or may in the future file for registration of such trademarks. If they succeed in registering or developing common law rights in such trademarks, and if we are not successful in challenging such third-party rights, we may not be able to use these trademarks to market our products in those countries. In any case, if we are unable to establish name recognition based on our trademarks and trade names, then we may not be able to compete effectively and our business may be adversely affected.
If we cannot show access and copying then our copyrights may not provide protection for our software and our business may be adversely affected.
Copyrights protect works of authorship such as software, but proving infringement requires a showing of access to the work and copying of the work. Because software is not readily available or accessible, it may be difficult to determine and prove that a third party had access to our software and/or that they copied our software. Because our software may be accessible by obtaining or accessing our product offerings and technology, third parties may be able to download or reproduce our software and reverse engineer our software programs. Software programs can be rewritten in ways that significantly modify it from the original program, which may make it difficult to prove the copying prong of a copyright infringement showing. If we are unable to establish the two prongs of a copyright infringement analysis, then our copyrights may provide limited or no protection for our software. Copyright infringement suits are expensive and any damages we seek may be inadequate to compensate us for the costs of litigation and for damage to our business resulting from the copyright infringement.
41
Table of Contents
We may not be able to adequately protect our intellectual property rights throughout the world.
Filing, prosecuting and defending patents on our products in all countries throughout the world would be prohibitively expensive. The requirements for patentability may differ in certain countries, particularly developing countries, and the breadth of patent claims allowed can be inconsistent. In addition, the laws of some foreign countries may not protect our intellectual property rights to the same extent as laws in the United States. Consequently, we may not be able to prevent third parties from practicing our inventions in all countries outside the United States. Competitors may use our technologies in jurisdictions where we have not obtained patent protection to develop their own products and, further, may export otherwise infringing products to territories in which we have patent protection that may not be sufficient to terminate infringing activities.
We do not have patent rights in certain foreign countries in which a market may exist. Moreover, in foreign jurisdictions where we do have patent rights, proceedings to enforce such rights could result in substantial costs and divert our efforts and attention from other aspects of our business, could put our patents at risk of being invalidated or interpreted narrowly, and our patent applications at risk of not issuing. Additionally, such proceedings could provoke third parties to assert claims against us. We may not prevail in any lawsuits that we initiate and the damages or other remedies awarded, if any, may not be commercially meaningful. Thus, we may not be able to stop a competitor from marketing and selling in foreign countries products and services that are the same as or similar to our products and services, and our competitive position in the international market would be harmed.
We may not identify relevant third-party patents or may incorrectly interpret the relevance, scope or expiration of a third-party patent which might adversely affect our ability to develop and market our products.
We cannot guarantee that any of our or our licensors’ patent searches or analyses, including the identification of relevant patents, the scope of patent claims or the expiration of relevant patents, are complete or thorough, nor can we be certain that we have identified each and every third-party patent and pending application in the United States and abroad that is relevant to or necessary for the commercialization of our products in any jurisdiction. For example, U.S. patent applications filed before November 29, 2000 and certain U.S. patent applications filed after that date that will not be filed outside the United States remain confidential until patents issue. Patent applications in the United States and elsewhere are published approximately 18 months after the earliest filing for which priority is claimed, with such earliest filing date being commonly referred to as the priority date. Therefore, patent applications covering our products could have been filed by others without our knowledge. Additionally, pending patent applications that have been published can, subject to certain limitations, be later amended in a manner that could cover our product candidates or the use of our products. The scope of a patent claim is determined by an interpretation of the law, the written disclosure in a patent and the patent’s prosecution history. Our interpretation of the relevance or the scope of a patent or a pending application may be incorrect, which may negatively impact our ability to market our products. We may incorrectly determine that our products are not covered by a third-party patent or may incorrectly predict whether a third party’s pending patent application will issue with claims of relevant scope. Our determination of the expiration date of any patent in the United States or abroad that we consider relevant may be incorrect, which may negatively impact our ability to develop and market our products and services. Our failure to identify and correctly interpret relevant patents may negatively impact our ability to develop and market our products and services.
If we fail to identify and correctly interpret relevant patents, we may be subject to infringement claims. We cannot guarantee that we will be able to successfully settle or otherwise resolve such infringement claims. If we fail in any such dispute, in addition to being forced to pay damages, we may be temporarily or permanently prohibited from commercializing any of our products that are held to be infringing. We might, if possible, also be forced to redesign products or services so that we no longer infringe the third-
42
Table of Contents
party intellectual property rights. Any of these events, even if we were ultimately to prevail, could require us to divert substantial financial and management resources that we would otherwise be able to devote to our business.
Patent terms may be inadequate to protect our competitive position on our products for an adequate amount of time.
Patents have a limited lifespan, and the protection patents afford is limited. In the United States, if all maintenance fees are timely paid, the natural expiration of a patent is generally 20 years from its earliest U.S. non-provisional filing date. Even if patents covering our products are obtained, once the patent life has expired for patents covering a product, we may be open to competition from competitive products and services. As a result, our patent portfolio may not provide us with sufficient rights to exclude others from commercializing product candidates similar or identical to ours.
Intellectual property rights do not necessarily address all potential threats to our business.
Once granted, patents may remain open to invalidity challenges including opposition, interference, re-examination, post-grant review, inter partes review, nullification or derivation action in court or before patent offices or similar proceedings for a given period after allowance or grant, during which time third parties can raise objections against such grant. In the course of such proceedings, which may continue for a protracted period of time, the patent owner may be compelled to limit the scope of the allowed or granted claims thus attacked, or may lose the allowed or granted claims altogether.
In addition, the degree of future protection afforded by our intellectual property rights is uncertain because even granted intellectual property rights have limitations, and may not adequately protect our business, provide a barrier to entry against our competitors or potential competitors or permit us to maintain our competitive advantage. Moreover, if a third party has intellectual property rights that cover the practice of our technology, we may not be able to fully exercise or extract value from our intellectual property rights. The following examples are illustrative:
| • | others may be able to develop and/or practice technology that is similar to our technology or aspects of our technology, but that are not covered by the claims of the patents that we own or control, assuming such patents have issued or do issue; |
| • | we or our licensors or any future strategic partners might not have been the first to conceive or reduce to practice the inventions covered by the issued patents or pending patent applications that we own or have exclusively licensed; |
| • | we or our licensors or any future strategic partners might not have been the first to file patent applications covering certain of our inventions; |
| • | others may independently develop similar or alternative technologies or duplicate any of our technologies without infringing our intellectual property rights; |
| • | it is possible that our pending patent applications will not lead to issued patents; |
| • | issued patents that we own or have exclusively licensed may not provide us with any competitive advantage, or may be held invalid or unenforceable, as a result of legal challenges by our competitors; |
| • | our competitors might conduct research and development activities in countries where we do not have patent rights and then use the information learned from such activities to develop competitive products for sale in our major commercial markets; |
| • | third parties performing manufacturing or testing for us using our products or technologies could use the intellectual property of others without obtaining a proper license; |
43
Table of Contents
| • | parties may assert an ownership interest in our intellectual property and, if successful, such disputes may preclude us from exercising exclusive rights over that intellectual property; |
| • | we may not develop or in-license additional proprietary technologies that are patentable; |
| • | we may not be able to obtain and maintain necessary licenses on commercially reasonable terms, or at all; and |
| • | the patents of others may have an adverse effect on our business. |
Should any of these events occur, they could significantly harm our business and results of operations.
We may be subject to claims that our employees, consultants or independent contractors have wrongfully used or disclosed confidential information of their former employers or other third parties.
We do and may employ individuals who were previously employed at universities or other pharmaceutical or medical device companies, including our licensors, competitors or potential competitors. Although we try to ensure that our employees, consultants and independent contractors do not use the proprietary information or know-how of others in their work for us, and we are not currently subject to any claims that our employees, consultants or independent contractors have wrongfully used or disclosed confidential information of third parties, we may in the future be subject to such claims. Litigation may be necessary to defend against these claims. If we fail in defending any such claims, in addition to paying monetary damages, we may lose valuable intellectual property rights or personnel. Such intellectual property rights could be awarded to a third party, and we could be required to obtain a license from such third party to commercialize our technology or products. Such a license may not be available on commercially reasonable terms or at all. Even if we are successful in defending against such claims, litigation could result in substantial costs and be a distraction to management and other employees, and could result in customers seeking other sources for the technology, or in ceasing from doing business with us.
Our intellectual property agreements with third parties may be subject to disagreements over contract interpretation, which could narrow the scope of our rights to the relevant intellectual property or technology.
Certain provisions in our intellectual property agreements may be susceptible to multiple interpretations. The resolution of any contract interpretation disagreement that may arise could affect the scope of our rights to the relevant intellectual property or technology, or affect financial or other obligations under the relevant agreement, either of which could have a material adverse effect on our business, financial condition, results of operations and prospects.
In addition, while it is our policy to require our employees and contractors who may be involved in the conception or development of intellectual property to execute agreements assigning such intellectual property to us, we may be unsuccessful in executing such an agreement with each party who in fact conceives or develops intellectual property that we regard as our own. Our assignment agreements may not be self-executing or may be breached, and we may be forced to bring claims against third parties, or defend claims they may bring against us, to determine the ownership of what we regard as our intellectual property.
We may not be successful in obtaining necessary intellectual property rights to future products through acquisitions and in-licenses.
Although we intend to develop products and technology through our own internal research, we may also seek to acquire or in-license technologies to grow our product offerings and technology portfolio. However, we may be unable to acquire or in-license intellectual property rights relating to, or necessary for, any such products or technology from third parties on commercially reasonable terms or at all. In
44
Table of Contents
that event, we may be unable to develop or commercialize such products or technology. We may also be unable to identify products or technology that we believe are an appropriate strategic fit for our company and protect intellectual property relating to, or necessary for, such products and technology.
The in-licensing and acquisition of third-party intellectual property rights for product candidates is a competitive area, and a number of more established companies are also pursuing strategies to in-license or acquire third-party intellectual property rights for products that we may consider attractive or necessary. These established companies may have a competitive advantage over us due to their size, cash resources and greater clinical development and commercialization capabilities. Furthermore, companies that perceive us to be a competitor may be unwilling to assign or license rights to us. If we are unable to successfully obtain rights to additional technologies or products, our business, financial condition, results of operations and prospects for growth could suffer.
In addition, we expect that competition for the in-licensing or acquisition of third-party intellectual property rights for products and technologies that are attractive to us may increase in the future, which may mean fewer suitable opportunities for us as well as higher acquisition or licensing costs. We may be unable to in-license or acquire the third-party intellectual property rights for products or technology on terms that would allow us to make an appropriate return on our investment.
Risks Related to Regulation of our Industry
Our future success depends on our ability to develop, receive regulatory clearance or approval for, and introduce new products or product enhancements that will be accepted by the market in a timely manner.
It is important to our business that we build a pipeline of product offerings for treatment of our target indications. As such, our success will depend in part on our ability to develop and introduce new products. However, we may not be able to successfully develop and obtain regulatory clearance or approval for product enhancements, or new products, or these products may not be accepted by physicians or the payors who financially support many of the procedures performed with our products.
The success of any new product offering or enhancement to an existing product will depend on a number of factors, including our ability to:
| • | identify and anticipate physician and patient needs properly; |
| • | develop and introduce new products or product enhancements in a timely manner; |
| • | avoid infringing upon the intellectual property rights of third parties; |
| • | demonstrate, if required, the safety and efficacy of new products with data from preclinical and clinical studies; |
| • | obtain the necessary regulatory clearances or approvals for new products or product enhancements; |
| • | comply fully with FDA and foreign regulations on marketing of new devices or modified products; |
| • | provide adequate training to potential users of our products; and |
| • | receive adequate coverage and reimbursement for procedures performed with our products. |
If we do not develop new products or product enhancements in time to meet market demand or if there is insufficient demand for these products or enhancements, or if our competitors introduce new products with functionalities that are superior to ours, our results of operations will suffer.
45
Table of Contents
gammaCore is subject to extensive governmental regulation, and our failure to comply with applicable requirements could cause our business to suffer.
The medical device industry is regulated extensively by governmental authorities, principally the FDA and corresponding state and foreign regulatory agencies and authorities, such as the EU legislative bodies and the EEA Member States, Competent Authorities and notified bodies. The FDA and other U.S., EEA and foreign governmental agencies and authorities regulate and oversee, among other things, with respect to medical devices:
| • | design, development and manufacturing; |
| • | testing, labeling, content and language of instructions for use and storage; |
| • | clinical trials; |
| • | product safety; |
| • | risk assessment and management; |
| • | marketing, sales and distribution; |
| • | pre-market regulatory clearance and approval; |
| • | conformity assessment procedures; |
| • | record-keeping procedures; |
| • | advertising and promotion; |
| • | recalls and other field safety corrective actions; |
| • | post-market surveillance, including reporting of deaths or serious injuries and malfunctions that, if they were to recur, could lead to death or serious injury; |
| • | post-market studies; and |
| • | product import and export. |
The laws and regulations to which we are subject are complex and have tended to become more stringent over time. Legislative or regulatory changes could result in restrictions on our ability to carry on or expand our operations, higher than anticipated costs or lower than anticipated sales.
Our failure to comply with U.S. federal and state regulations or EEA or other foreign regulations applicable in the countries where we operate could lead to the issuance of warning letters or untitled letters, the imposition of injunctions, suspensions or loss of regulatory clearance or approvals, product recalls, termination of distribution, product seizures or civil penalties. In the most extreme cases, criminal sanctions or closure of our manufacturing facilities are possible. If any of these risks materialize, our business would be adversely affected.
gammaCore is also subject to extensive governmental regulation in foreign jurisdictions, such as Europe, and our failure to comply with applicable requirements could cause our business to suffer.
In the EEA, gammaCore must comply with the Essential Requirements laid down in Annex I to Directive 93/42/EEC on the approximation of the laws of the Member States relating to medical devices or the EU Medical Devices Directive. Compliance with these requirements is a prerequisite to be able to affix the CE mark to gammaCore, without which they cannot be marketed or sold in the EEA. To demonstrate compliance with the Essential Requirements and obtain the right to affix the CE Mark medical devices manufacturers must undergo a conformity assessment procedure, which varies according to the type of medical device and its classification. Except for low risk medical devices (Class I with no measuring function and which are not sterile), where the manufacturer can issue an EC Declaration of Conformity
46
Table of Contents
based on a self-assessment of the conformity of its products with the Essential Requirements, a conformity assessment procedure requires the intervention of a Notified Body, which is an organization designated by a competent authority of an EEA country to conduct conformity assessments. Depending on the relevant conformity assessment procedure, the Notified Body would audit and examine the Technical File and the quality system for the manufacture, design and final inspection of the medical devices. The Notified Body issues a CE Certificate of Conformity following successful completion of a conformity assessment procedure conducted in relation to the medical device and its manufacturer and their conformity with the Essential Requirements. This Certificate entitles the manufacturer to affix the CE mark to its medical devices after having prepared and signed a related EC Declaration of Conformity.
As a general rule, demonstration of conformity of medical devices and their manufacturers with the Essential Requirements must be based, among other things, on the evaluation of clinical data supporting the safety and performance of the products during normal conditions of use. Specifically, a manufacturer must demonstrate that the device achieves its intended performance during normal conditions of use and that the known and foreseeable risks, and any adverse events, are minimized and acceptable when weighed against the benefits of its intended performance, and that any claims made about the performance and safety of the device, such as product labeling and instructions for use, are supported by suitable evidence. This assessment must be based on clinical data, which can be obtained from (1) clinical studies conducted on the devices being assessed, (2) scientific literature from similar devices whose equivalence with the assessed device can be demonstrated or (3) both clinical studies and scientific literature. With respect to Class III devices, the manufacturer must conduct clinical studies to obtain the required clinical data, unless reliance on existing clinical data from equivalent devices can be justified. The conduct of clinical studies in the EEA is governed by detailed regulatory obligations. These may include the requirement of prior authorization by the competent authorities of the country in which the study takes place and the requirement to obtain a positive opinion from a competent Ethics Committee. This process can be expensive and time-consuming.
Moreover, on May 25, 2017 the new Medical Devices Regulation (2017/745 or MDR) entered into force. Following its entry into application on May 26, 2020, the Regulations will introduce substantial changes to the obligations with which medical device manufacturers must comply in the EU. High risk medical devices will be subject to additional scrutiny during the conformity assessment procedure. Specifically, the EU Medical Devices Regulation repeals and replaces the EU Medical Devices Directive. Unlike directives, which must be implemented into the national laws of the EEA Member States, the regulations would be directly applicable, i.e., without the need for adoption of EEA Member State laws implementing them, in all EEA Member States and are intended to eliminate current differences in the regulation of medical devices among EEA Member States. The EU Medical Devices Regulation, among other things, is intended to establish a uniform, transparent, predictable and sustainable regulatory framework across the EEA for medical devices and ensure a high level of safety and health while supporting innovation. The EU Medical Devices Regulation will however only become applicable three years after publication (in May 2020). Once applicable, the new regulations will among other things:
| • | strengthen the rules on placing devices on the market and reinforce surveillance once they are available; |
| • | establish explicit provisions on manufacturers’ responsibilities for the follow-up of the quality, performance and safety of devices placed on the market; |
| • | improve the traceability of medical devices throughout the supply chain to the end-user or patient through a unique identification number; |
| • | set up a central database to provide patients, healthcare professionals and the public with comprehensive information on products available in the EU; and |
| • | strengthened rules for the assessment of certain high-risk devices which may have to undergo an additional check by experts before they are placed on the market. |
47
Table of Contents
Once applicable, the Medical Devices Regulation may impose increased compliance obligations for us to access the EU market.
In order to continue to sell gammaCore in Europe, we must maintain our CE Mark and continue to comply with certain EU Directives and, in the future with the EU Medical Devices Regulation. Our failure to continue to comply with applicable foreign regulatory requirements, including those administered by authorities of the EEA countries, could result in enforcement actions against us, including refusal, suspension or withdrawal of our CE Certificates of Conformity by our Notified Body (the British Standards Institution, or BSI), which could impair our ability to market products in the EEA in the future.
If we fail to maintain regulatory approvals and clearances, or are unable to obtain, or experience significant delays in obtaining, FDA clearances or approvals for our future products or product enhancements, our ability to commercially distribute and market these products could suffer.
Our products are subject to rigorous regulation by the FDA and numerous other federal, state and foreign governmental authorities. The process of obtaining regulatory clearances or approvals to market a medical device can be costly and time consuming, and we may not be able to obtain these clearances or approvals on a timely basis, if at all. In particular, the FDA permits commercial distribution of a new medical device only after the device has received clearance under Section 510(k) of the Federal Food, Drug and Cosmetic Act, or is the subject of an approved premarket approval application, or PMA unless the device is specifically exempt from those requirements. The FDA will clear marketing of a lower risk medical device through the 510(k) process if the manufacturer demonstrates that the new product is substantially equivalent to a legally marketed “predicate” device. High risk devices deemed to pose the greatest risk, such as life-sustaining, life-supporting, or implantable devices, or devices not deemed substantially equivalent to a legally marketed “predicate” device, require the approval of a PMA. The PMA process is more costly, lengthy and uncertain than the 510(k) clearance process. A PMA application must be supported by extensive data, including, but not limited to, technical, preclinical, clinical trial, manufacturing and labeling data, to demonstrate to the FDA’s satisfaction the safety and efficacy of the device for its intended use. Our currently commercialized gammaCore products have been cleared through the 510(k) process. However, we may need to submit a PMA to expand our labeling claims to include certain indications.
Our failure to comply with U.S. federal, state and foreign governmental regulations could lead to the issuance of warning letters or untitled letters, the imposition of injunctions, suspensions or loss of regulatory clearance or approvals, product recalls, termination of distribution, product seizures or civil penalties. In the most extreme cases, criminal sanctions or closure of our manufacturing facility are possible.
Foreign governmental authorities that regulate the manufacture and sale of medical devices have become increasingly stringent and, to the extent we market and sell our products internationally, we may be subject to rigorous international regulation in the future. In these circumstances, we would rely significantly on our foreign independent distributors to comply with the varying regulations, and any failures on their part could result in restrictions on the sale of our products in foreign countries.
Modifications to our products may require new regulatory clearances or approvals or may require us to recall or cease marketing our products until clearances or approvals are obtained.
Modifications to or expansion of our indications for use of our gammaCore products may require new regulatory approvals or clearances, including 510(k) clearances or PMA approvals, or require us to recall or cease marketing the modified devices until these clearances or approvals are obtained. The FDA requires device manufacturers to initially make and document a determination of whether or not a
48
Table of Contents
modification requires a new approval, supplement or clearance. A manufacturer may determine that a modification does not significantly affect safety or efficacy and does not represent a major change in its intended use, so that no new 510(k) clearance is not necessary. However, the FDA can review a manufacturer’s decision and may disagree. The FDA may also on its own initiative determine that a new clearance or approval is required. We may make modifications to our products in the future that we believe do not or will not require additional clearances or approvals. If the FDA disagrees and requires new clearances or approvals for the modifications, we may be required to recall and to stop marketing our products as modified, which could require us to redesign our products and harm our operating results. In these circumstances, we may be subject to significant enforcement actions.
If a manufacturer determines that a modification to an FDA-cleared device could significantly affect its safety or efficacy, or would constitute a major change in its intended use, then the manufacturer must file for a new 510(k) clearance or possibly a PMA application. Where we determine that modifications to our products require a new 510(k) clearance or PMA application, we may not be able to obtain those additional clearances or approvals for the modifications or additional indications in a timely manner, or at all. For those products sold in the EU, we must notify our E.U. Notified Body, if significant changes are made to the products or if there are substantial changes to our quality assurance systems affecting those products. Obtaining clearances and approvals can be a time consuming process, and delays in obtaining required future clearances or approvals would adversely affect our ability to introduce new or enhanced products in a timely manner, which in turn would harm our future growth.
There is no guarantee that the FDA will grant 510(k) clearance or PMA approval of our future products and failure to obtain necessary clearances or approvals for our future products would adversely affect our ability to grow our business.
Some of our new products or expanded indications for use will require FDA clearance of a 510(k), or may require FDA approval of a PMA. The FDA may not approve or clear these products for the indications that are necessary or desirable for successful commercialization. Indeed, the FDA may refuse our requests for 510(k) clearance or premarket approval of new products, new intended uses or modifications to existing products. Failure to receive clearance or approval for our new products would have an adverse effect on our ability to expand our business.
Even if our products are cleared or approved by regulatory authorities, if we or our suppliers fail to comply with ongoing FDA or other foreign regulatory authority requirements, or if we experience unanticipated problems with our products, these products could be subject to restrictions or withdrawal from the market.
Any product for which we obtain clearance or approval, and the manufacturing processes, reporting requirements, post-approval clinical data and promotional activities for such product, will be subject to continued regulatory review, oversight and periodic inspections by the FDA and other domestic and foreign regulatory bodies. In particular, we and our suppliers are required to comply with FDA’s Quality System Regulation, or QSR, and International Standards Organization, or ISO, regulations for the manufacture of our products and other regulations which cover the methods and documentation of the design, testing, production, control, quality assurance, labeling, packaging, storage and shipping of any product for which we obtain clearance or approval. Regulatory bodies, such as the FDA, enforce the QSR and other regulations through periodic inspections. The failure by us or one of our suppliers to comply with applicable statutes and regulations administered by the FDA and other regulatory bodies, or the failure to timely and adequately respond to any adverse inspectional observations or product safety issues, could result in, among other things, any of the following enforcement actions:
| • | untitled letters, warning letters, fines, injunctions, consent decrees and civil penalties; |
| • | unanticipated expenditures to address or defend such actions |
| • | customer notifications for repair, replacement, refunds; |
49
Table of Contents
| • | recall, detention or seizure of our products; |
| • | operating restrictions or partial suspension or total shutdown of production; |
| • | refusing or delaying our requests for 510(k) clearance or PMA approval of new products or modified products; |
| • | operating restrictions; |
| • | withdrawing 510(k) clearances on PMA approvals that have already been granted; |
| • | refusal to grant export approval for our products; or |
| • | criminal prosecution. |
If any of these actions were to occur it would harm our reputation and cause our product sales and profitability to suffer and may prevent us from generating revenue. Furthermore, our key component suppliers may not currently be or may not continue to be in compliance with all applicable regulatory requirements which could result in our failure to produce our products on a timely basis and in the required quantities, if at all.
Even if regulatory clearance or approval of a product is granted, such clearance or approval may be subject to limitations on the intended uses for which the product may be marketed and reduce our potential to successfully commercialize the product and generate revenue from the product. If the FDA determines that our promotional materials, labeling, training or other marketing or educational activities constitute promotion of an unapproved use, it could request that we cease or modify our training or promotional materials or subject us to regulatory enforcement actions. It is also possible that other federal, state or foreign enforcement authorities might take action if they consider our training or other promotional materials to constitute promotion of an unapproved use, which could result in significant fines or penalties under other statutory authorities, such as laws prohibiting false claims for reimbursement.
In addition, we may be required to conduct costly post-market testing and surveillance to monitor the safety or effectiveness of our products, and we must comply with medical device reporting, or MDR, requirements, including the reporting of adverse events and malfunctions related to our products. Later discovery of previously unknown problems with our products, including unanticipated adverse events or adverse events of unanticipated severity or frequency, manufacturing problems, or failure to comply with regulatory requirements such as QSR may result in changes to labeling, restrictions on such products or manufacturing processes, withdrawal of the products from the market, voluntary or mandatory recalls, a requirement to repair, replace or refund the cost of any medical device we manufacture or distribute, fines, suspension of regulatory clearances or approvals, product seizures, injunctions or the imposition of civil or criminal penalties which would adversely affect our business, operating results and prospects.
The misuse or off-label use of our gammaCore therapy may harm our image in the marketplace, result in injuries that lead to product liability suits, which could be costly to our business, or result in costly investigations and sanctions from the FDA and other regulatory bodies if we are deemed to have engaged in off-label promotion.
gammaCore has been CE Marked in the EEA and cleared by the FDA for the acute treatment of eCH and the acute treatment of migraine headache in the United States. We may only promote or market our gammaCore therapy for its specifically approved indications as described on the approved label. We train our marketing and sales force against promoting our products for uses outside of the approved indications for use, known as “off-label uses.” We cannot, however, prevent a physician from prescribing our product off-label, when in the physician’s independent professional medical judgment he or she deems appropriate. There may be increased risk of injury to patients if patients attempt to use our
50
Table of Contents
product off-label. Furthermore, the use of our product for indications other than those cleared or approved by the applicable regulatory body may not effectively treat such conditions, which could harm our reputation in the marketplace among physicians and patients.
Patients may also misuse our product or use improper techniques if they are not adequately trained, potentially leading to injury and an increased risk of product liability. If our product is misused or used with improper technique, we may become subject to costly litigation by our customers or their patients. Product liability claims could divert management’s attention from our core business, be expensive to defend, and result in sizable damage awards against us that may not be covered by insurance. In addition, if our products are approved for sale in the United States and the FDA determines that our promotional materials or training constitute promotion of an off-label use, it could request that we modify our training or promotional materials or subject us to regulatory or enforcement actions, including the issuance of an untitled letter, a warning letter, injunction, seizure, civil fine or criminal penalties. It is also possible that other federal, state or foreign enforcement authorities might take action if they consider our business activities to constitute promotion of an off-label use, which could result in significant penalties, including, but not limited to, criminal, civil and/or administrative penalties, damages, fines, disgorgement, exclusion from participation in government healthcare programs, and the curtailment of our operations. Further, our competitors could bring civil actions under relevant unfair competition and advertising laws should they believe our business activities and product promotional activities are improper. Any of these events could significantly harm our business and results of operations and cause our stock price to decline.
Further, the advertising and promotion of our products is subject to EEA Member States’ national laws implementing Directive 93/42/EEC on the approximation of the laws of the Member States relating to medical devices, Directive 2006/114/EC concerning misleading and comparative advertising, and Directive 2005/29/EC on unfair commercial practices, as well as other EEA Member State legislation governing the advertising and promotion of medical devices. EEA Member State legislation may also restrict or impose limitations on our ability to advertise our products directly to the general public. In addition, voluntary EU and national Codes of Conduct provide guidelines on the advertising and promotion of our products to the general public and may impose limitations on our promotional activities with healthcare professionals.
gammaCore may in the future be subject to notifications, recalls, or voluntary market withdrawals that could harm our reputation, business and financial results.
The FDA, EEA Competent Authorities and similar foreign governmental authorities have the authority to request or require the recall of commercialized products in the event of regulatory noncompliance or material deficiencies or defects in design or manufacture that could affect patient safety. In the case of the FDA, the authority to require a recall must be based on an FDA finding that there is a reasonable probability that the device would cause serious injury or death. In addition, foreign governmental bodies have the authority to require the recall of our products in the event of material deficiencies or defects in design or manufacture. Manufacturers may, under their own initiative, recall a product if any material deficiency in a device is found. A government-mandated or voluntary recall by us or one of our distributors could occur as a result of component failures, manufacturing errors, design or labeling defects or other deficiencies and issues. Recalls of any of our products would divert managerial and financial resources and have an adverse effect on our financial condition and results of operations. We must notify the FDA of all device recalls and corrections, and certain classifications of recalls and corrections require more extensive reporting within 10 working days after the recall is initiated. Companies are required to maintain certain records of recalls and corrections, even if they are not subject to more extensive reporting requirements. We may initiate voluntary market withdrawals or other market actions involving our gammaCore products in the future that we determine do not require notification of the FDA. If the FDA disagrees with our determinations, they could require us to report
51
Table of Contents
those actions as recalls. A future recall announcement could harm our reputation with customers and negatively affect our sales. In addition, the FDA could take enforcement action for failing to report the recalls or corrections when they were conducted. Consumer class action claims and/or product liability claims are a greater risk following a product recall or market withdrawal.
We are required to report certain malfunctions, deaths, and serious injuries associated with our products, which can result in voluntary corrective actions or agency enforcement actions.
Under the FDA MDR regulations, medical device manufacturers are required to submit information to the FDA when they receive a report or become aware that a device has or may have caused or contributed to a death or serious injury or has or may have a malfunction that would likely cause or contribute to death or serious injury if the malfunction were to recur. All manufacturers placing medical devices on the market in the EEA are legally bound to report incidents involving devices they produce or sell to the regulatory agency, or competent authority, in whose jurisdiction the incident occurred. Under the Directive 93/42/EEC on the approximation of the laws of the Member States relating to medical devices, an incident is defined as any malfunction or deterioration in the characteristics and/or performance of a device, as well as any inadequacy in the labeling or the instructions for use which, directly or indirectly, might lead to or might have led to the death of a patient, or user or of other persons or to a serious deterioration in their state of health.
Malfunction of our products could result in future voluntary corrective actions, such as recalls, including corrections, or customer notifications, or agency action, such as inspection or enforcement actions. If malfunctions do occur, we may be unable to correct the malfunctions adequately or prevent further malfunctions, in which case we may need to cease manufacture and distribution of the affected products, initiate voluntary recalls, and redesign the products. Regulatory authorities may also take actions against us, such as ordering recalls, imposing fines, or seizing the affected products. Any corrective action, whether voluntary or involuntary, will require the dedication of our time and capital, distract management from operating our business, and may harm our reputation and financial results.
Legislative or regulatory reforms may make it more difficult and costly for us to obtain regulatory approval of our product candidates and to manufacture, market and distribute our products after approval is obtained.
From time to time, legislation is drafted and introduced in Congress that could significantly change the statutory provisions governing the regulatory approval, manufacture and marketing of regulated products or the reimbursement thereof. In addition, FDA regulations and guidance are often revised or reinterpreted by the FDA in ways that may significantly affect our business and our products. Any new regulations or revisions or reinterpretations of existing regulations may impose additional costs or lengthen review times of future products. It is impossible to predict whether legislative changes will be enacted or FDA regulations, guidance or interpretations changed, and what the impact of such changes, if any, may be.
Moreover, the policies of the Trump Administration and their impact on the regulation of our products in the United States remain uncertain. The outcome of the 2016 election and the forthcoming 2018 mid-term elections could result in significant legislative and regulatory reforms impacting the FDA’s regulation of our products. Any change in the laws or regulations that govern the clearance and approval processes relating to our current and future products could make it more difficult and costly to obtain clearance or approval for new products, or to produce, market and distribute existing products. Significant delays in receiving clearance or approval, or the failure to receive clearance or approval for our new products would have an adverse effect on our ability to expand our business.
In the EU, on May 25, 2017 the new Medical Devices Regulation (2017/745 or MDR) was adopted. Following its entry into application on May 26, 2020, the Regulations will introduce substantial changes
52
Table of Contents
to the obligations with which medical device manufacturers must comply in the EU. High risk medical devices will be subject to additional scrutiny during the conformity assessment procedure.
We are subject to federal, state and foreign healthcare laws and regulations, and a finding of failure to comply with such laws and regulations could have a material adverse effect on our business.
We are subject to healthcare fraud and abuse regulation and enforcement by federal, state and foreign governments, which could significantly impact our business. In the United States, the laws that may affect our ability to operate include, but are not limited to:
| • | the federal Anti-Kickback Statute, which prohibits, among other things, persons and entities from knowingly and willfully soliciting, receiving, offering, or paying remuneration, directly or indirectly, in cash or in kind, in exchange for or to induce either the referral of an individual for, or the purchase, lease, order or recommendation of, any good, facility, item or service for which payment may be made, in whole or in part, under federal healthcare programs such as Medicare and Medicaid. A person or entity does not need to have actual knowledge of this statute or specific intent to violate it in order to have committed a violation. Moreover, the government may assert that a claim including items or services resulting from a violation of the federal Anti-Kickback Statute constitutes a false or fraudulent claim for purposes of the federal civil False Claims Act. Violations of the federal Anti-Kickback Statute may result in civil monetary penalties up to $74,792 for each violation, plus up to three times the remuneration involved. Civil penalties for such conduct can further be assessed under the federal False Claims Act. Violations can also result in criminal penalties, including criminal fines of up to $100,000 and imprisonment of up to 10 years. Similarly, violations can result in exclusion from participation in government healthcare programs, including Medicare and Medicaid; |
| • | In the event that third-party payors require us to be a durable medical equipment, or DME, supplier or we sell our products directly to providers who are DME suppliers that submit claims to such payors, we may be subject to the federal Stark physician self-referral law, which prohibits a physician from making a referral for certain designated health services covered by the Medicare program, including DME, if the physician or an immediate family member has a financial relationship with the entity providing the designated health services, and prohibits that entity from billing or presenting a claim for the designated health services furnished pursuant to the prohibited referral, unless an exception applies. Sanctions for violating the Stark Law include denial of payment, civil monetary penalties of up to $24,253 per claim submitted and exclusion from the federal health care programs. Failure to refund amounts received as a result of a prohibited referral on a timely basis may constitute a false or fraudulent claim and may result in civil penalties and additional penalties under the FCA. The statute also provides for a penalty of up to $161,692 for a circumvention scheme. Various states also have corollary laws to the Stark Law, including laws that require physicians to disclose any financial interest they may have with a healthcare provider to their patients when referring patients to that provider. Both the scope and exceptions for such laws vary from state to state. |
| • | federal civil and criminal false claims laws and civil monetary penalty laws, including civil whistleblower or qui tam actions, that prohibit, among other things, knowingly presenting, or causing to be presented, claims for payment or approval to the federal government that are false or fraudulent, knowingly making a false statement material to an obligation to pay or transmit money or property to the federal government or knowingly concealing or knowingly and improperly avoiding or decreasing an obligation to pay or transmit money or property to the federal government. These laws can apply to manufacturers who provide information on coverage, coding, and reimbursement of their products to persons who bill third-party payors. Private individuals can bring False Claims Act “qui tam” actions, on |
53
Table of Contents
| behalf of the government and such individuals, commonly known as “whistleblowers,” may share in amounts paid by the entity to the government in fines or settlement. When an entity is determined to have violated the federal civil False Claims Act, the government may impose civil fines and penalties ranging from $11,181 to $22,363 for each false claim, plus treble damages, and exclude the entity from participation in Medicare, Medicaid and other federal healthcare programs; |
| • | the federal Health Insurance Portability and Accountability Act of 1996, or HIPAA, which created federal criminal laws that prohibit executing a scheme to defraud any healthcare benefit program or making false statements relating to healthcare matters. A person or entity does not need to have actual knowledge of these statutes or specific intent to violate them; |
| • | HIPAA, as amended by the Health Information Technology for Economic and Clinical Health Act of 2009, or HITECH, and their respective implementing regulations, which impose requirements on certain covered healthcare providers, health plans and healthcare clearinghouses as well as their business associates that perform services for them that involve individually identifiable health information, relating to the privacy, security and transmission of individually identifiable health information without appropriate authorization, including mandatory contractual terms as well as directly applicable privacy and security standards and requirements. Failure to comply with the HIPAA privacy and security standards can result in civil monetary penalties up to $55,910 per violation, not to exceed $1.68 million per calendar year for non-compliance of an identical provision, and, in certain circumstances, criminal penalties with fines up to $250,000 per violation and/or imprisonment. State attorneys general can also bring a civil action to enjoin a HIPAA violation or to obtain statutory damages on behalf of residents of his or her state; |
| • | the federal physician sunshine requirements under the Patient Protection and Affordable Care Act, as amended by the Health Care and Education Reconciliation Act, or collectively, the ACA, which require certain applicable manufacturers of drugs, devices, biologics, and medical supplies for which payment is available under Medicare, Medicaid or the Children’s Health Insurance Program, or CHIP, to report annually to the U.S. Department of Health and Human Services Centers for Medicare and Medicaid Services, or CMS, information related to payments and other transfers of value to physicians (defined to include doctors, dentists, optometrists, podiatrists and chiropractors) and teaching hospitals, and ownership and investment interests held by physicians and their immediate family members. Applicable manufacturers are required to submit annual reports to CMS. Failure to submit required information may result in civil monetary penalties of $11,052 per failure up to an aggregate of $165,786 per year (or up to an aggregate of $1.105 million per year for “knowing failures”), for all payments, transfers of value or ownership or investment interests that are not timely, accurately, and completely reported in an annual submission, and may result in liability under other federal laws or regulations; and |
| • | state and foreign law equivalents of each of the above federal laws, such as state anti-kickback and false claims laws that may apply to items or services reimbursed by any third-party payor, including commercial insurers; state laws that require device companies to comply with the industry’s voluntary compliance guidelines and the relevant compliance guidance promulgated by the federal government, or otherwise restrict payments that may be made to healthcare providers and other potential referral sources; state laws that require device manufacturers to report information related to payments and other transfers of value to physicians and other healthcare providers or marketing expenditures; and state and foreign laws governing the privacy and security of health information in certain circumstances, many of which differ from each other in significant ways and often are not preempted by HIPAA. |
54
Table of Contents
These laws and regulations, among other things, constrain our business, marketing and other promotional activities by limiting the kinds of financial arrangements we may have with physicians or other entities or individuals in a position to prescribe or recommend our products. We have entered into consulting agreements and other arrangements with physicians, including some who have ownership interests in us and/or prescribe our products to patients. Compensation under some of these arrangements includes the provision of profits interests in our company. We could be adversely affected if regulatory agencies determine our financial relationships with such physicians to be in violation of applicable laws. Due to the breadth of these laws, the narrowness of statutory exceptions and regulatory safe harbors available, and the range of interpretations to which they are subject, it is possible that some of our current or future practices might be challenged under one or more of these laws.
The scope and enforcement of each of these laws is uncertain and subject to rapid change in the current environment of healthcare reform, especially in light of the lack of applicable precedent and regulations. Federal and state enforcement bodies have recently increased their scrutiny of interactions between healthcare companies and healthcare providers, which has led to a number of investigations, prosecutions, convictions and settlements in the healthcare industry. Responding to investigations can be time-and resource-consuming and can divert management’s attention from the business. Additionally, as a result of these investigations, healthcare providers and entities may have to agree to additional onerous compliance and reporting requirements as part of a consent decree or corporate integrity agreement. Any such investigation or settlement could increase our costs or otherwise have an adverse effect on our business.
If our operations are challenged or found to be in violation of any of the laws described above or any other governmental regulations that apply to us now or in the future, we may be subject to penalties, including civil and criminal penalties, damages, fines, disgorgement, exclusion from governmental health care programs, and the curtailment or restructuring of our operations, any of which could adversely affect our ability to operate our business and our financial results.
Healthcare legislative reform measures may have a material adverse effect on us.
In the United States, there have been and continue to be a number of legislative initiatives to contain healthcare costs. ACA, which was passed in 2010, substantially changed the way health care is financed by both governmental and private insurers and significantly impacts the U.S. healthcare industry. The ACA included, among other things, a deductible 2.3% excise tax on any entity that manufactures or imports medical devices offered for sale in the United States, with limited exceptions, effective January 1, 2013. Through a series of legislative amendments, the tax was suspended for 2016 through 2019. Absent further legislative action, the device excise tax will be reinstated on medical device sales starting January 1, 2020. This excise tax is resulting in a significant increase in the tax burden on our industry, and if any efforts we undertake to offset the excise tax are unsuccessful as we begin to sell the product in the United States, the increased tax burden could have an adverse effect on our results of operations and cash flows. Other elements of the ACA, including comparative effectiveness research, an independent payment advisory board and payment system reforms, including shared savings pilots and other provisions, may significantly affect the payment for, and the availability of, healthcare services and result in fundamental changes to federal healthcare reimbursement programs, any of which may materially affect numerous aspects of our business.
We do not yet know the full impact that the ACA will have on our business. The taxes imposed by the ACA and the expansion in the government’s role in the U.S. healthcare industry may result in decreased profits to us, lower reimbursement by payors for our products, and/or reduced medical procedure volumes, all of which may have a material adverse impact on our business, financial condition, results of operations, or cash flows. The Trump Administration and the U.S. Congress may take further action regarding the ACA, including, but not limited to, repeal or replacement. Most recently, the Tax Cuts and
55
Table of Contents
Jobs Acts was enacted, which, among other things, removes penalties for not complying with the individual mandate to carry health insurance. Additionally, all or a portion of the ACA and related subsequent legislation may be modified, repealed or otherwise invalidated through judicial challenge, which could result in lower numbers of insured individuals, reduced coverage for insured individuals and adversely affect our business.
In addition, other legislative changes have been proposed and adopted in the United States since the ACA was enacted. On August 2, 2011, the Budget Control Act of 2011 among other things includes aggregate reductions of Medicare payments to providers of 2% per fiscal year, which went into effect on April 1, 2013, and will remain in effect through 2025 unless additional Congressional action is taken. On January 2, 2013, the American Taxpayer Relief Act of 2012 was signed into law which, among other things, further reduced Medicare payments to certain providers, including hospitals.
We expect that additional state and federal healthcare reform measures will be adopted in the future, any of which could limit the amounts that federal and state governments will pay for healthcare products and services, which could result in reduced demand for our product candidates or additional pricing pressures.
Risks Related to Our Common Stock and This Offering
We will incur significantly increased costs and devote substantial management time as a result of operating as a public company.
As a public company, we will incur significant legal, accounting and other expenses that we did not incur as a private company. For example, we will be subject to the reporting requirements of the Exchange Act, and will be required to comply with the applicable requirements of the Sarbanes-Oxley Act of 2002, or the Sarbanes-Oxley Act, and the Dodd-Frank Wall Street Reform and Consumer Protection Act, as well as rules and regulations subsequently implemented by the Securities and Exchange Commission, or SEC, and Nasdaq, including the establishment and maintenance of effective disclosure and financial controls and changes in corporate governance practices. We expect that compliance with these requirements will increase our legal and financial compliance costs and will make some activities more time consuming and costly.
In addition, we expect that our management and other personnel will need to divert attention from operational and other business matters to devote substantial time to these public company requirements. In particular, we expect to incur significant expenses and devote substantial management effort toward ensuring compliance with the requirements of Section 404 of the Sarbanes-Oxley Act, which will increase when we are no longer an emerging growth company, as defined by the JOBS Act. We will need to hire additional accounting and financial staff with appropriate public company experience and technical accounting knowledge and may need to establish an internal audit function. We cannot predict or estimate the amount of additional costs we may incur as a result of becoming a public company or the timing of such costs. Additional compensation costs and any future equity awards will increase our compensation expense, which would increase our general and administrative expense and could adversely affect our profitability. We also expect that operating as a public company will make it more difficult and expensive for us to obtain director and officer liability insurance on reasonable terms. As a result, it may be more difficult for us to attract and retain qualified people to serve on our board of directors, our board committees or as executive officers.
56
Table of Contents
Our stock price may be volatile and you may not be able to resell shares of our common stock at or above the price you paid.
The trading price of our common stock following this offering could be highly volatile and could be subject to wide fluctuations in response to various factors, some of which are beyond our control. These factors include those discussed in this “Risk Factors” section of this prospectus and others such as:
| • | announcements related to regulatory clearance to market gammaCore for the treatment of various conditions in the United States; |
| • | results from, or any delays in, clinical trial programs relating to our product candidates; |
| • | announcements of new products by us or our competitors; |
| • | adverse actions taken by regulatory agencies with respect to our clinical trials, manufacturing supply chain or sales and marketing activities; |
| • | our operating results; |
| • | changes or developments in laws or regulations applicable to our products; |
| • | any adverse changes in our relationship with any manufacturers or suppliers; |
| • | the success of our efforts to acquire or develop additional products; |
| • | any intellectual property infringement actions in which we may become involved; |
| • | announcements concerning our competitors or the medical device industry in general; |
| • | achievement of expected product sales and profitability; |
| • | manufacture, supply or distribution shortages; |
| • | actual or anticipated fluctuations in our operating results; |
| • | FDA or other U.S. or foreign regulatory actions affecting us or our industry or other healthcare reform measures in the United States; |
| • | changes in financial estimates or recommendations by securities analysts; |
| • | trading volume of our common stock; |
| • | sales of our common stock by us, our executive officers and directors or our stockholders in the future; |
| • | general economic and market conditions and overall fluctuations in the U.S. equity markets; and |
| • | the loss of any of our key scientific or management personnel. |
In addition, the stock markets in general, and the markets for pharmaceutical and medical device stocks in particular, have experienced volatility. These broad market fluctuations may adversely affect the trading price or liquidity of our common stock. In the past, when the market price of a stock has been volatile, holders of that stock have sometimes instituted securities class action litigation against the issuer. If any of our stockholders were to bring such a lawsuit against us, we could incur substantial costs defending the lawsuit and the attention of our management would be diverted from the operation of our business, which could seriously harm our financial position. Any adverse determination in litigation could also subject us to significant liabilities.
57
Table of Contents
We have broad discretion to determine how to use the funds raised in this offering, and may use them in ways that may not enhance our operating results or the price of our common stock.
Our management will have broad discretion over the use of proceeds from this offering, and we could spend the proceeds from this offering in ways our stockholders may not agree with or that do not yield a favorable return, if at all. We currently expect to use the net proceeds from this offering for working capital and other corporate purposes including to (i) continue funding our activities related to the commercial launch of gammaCore initially for the acute treatment of migraine and eCH in the United States, (ii) invest in the expansion of gammaCore into additional indications in headache and rheumatology, and (iii) further build out our specialty pharmaceutical ecosystem. If we do not invest or apply the proceeds of this offering in ways that improve our operating results, we may fail to achieve expected financial results, which could cause our stock price to decline.
An active, liquid and orderly market for our common stock may not develop, and you may not be able to resell your common stock at or above the public offering price.
Prior to this offering, there was no public market for shares of our common stock, and an active public market for our shares may not develop or be sustained after this offering. We and the representatives of the underwriters have determined the initial public offering price of our common stock through negotiation. This price does not necessarily reflect the price at which investors in the market will be willing to buy and sell our shares following this offering. In addition, an active trading market may not develop following the consummation of this offering or, if it does develop, may not be sustained. The lack of an active market may impair your ability to sell your shares at the time you wish to sell them or at a price that you consider reasonable. An inactive market may also impair our ability to raise capital by selling shares and may impair our ability to acquire other businesses or technologies or in-license new product candidates using our shares as consideration.
If securities or industry analysts do not publish research or reports about our business, or if they issue an adverse or misleading opinion regarding our stock, our stock price and trading volume could decline.
The trading market for our common stock will be influenced by the research and reports that industry or securities analysts publish about us or our business. We do not currently have and may never obtain research coverage by securities and industry analysts. If no or few securities or industry analysts commence coverage of us, the trading price for our stock would be negatively impacted. In the event we obtain securities or industry analyst coverage, if any of the analysts who cover us issues an adverse or misleading opinion regarding us, our business model, our intellectual property or our stock performance, or if our clinical trials and operating results fail to meet the expectations of analysts, our stock price would likely decline. If one or more of these analysts cease coverage of us or fail to publish reports on us regularly, we could lose visibility in the financial markets, which in turn could cause our stock price or trading volume to decline.
We are an “emerging growth company” and as a result of the reduced disclosure and governance requirements applicable to emerging growth companies, our common stock may be less attractive to investors.
We are an “emerging growth company,” as defined in the JOBS Act, and we intend to take advantage of certain exemptions from various reporting requirements that are applicable to other public companies that are not emerging growth companies including, but not limited to, not being required to comply with the auditor attestation requirements of Section 404 of the Sarbanes-Oxley Act, reduced disclosure obligations regarding executive compensation in our periodic reports and proxy statements and exemptions from the requirements of holding a nonbinding advisory vote on executive compensation and stockholder approval of any golden parachute payments not previously approved. We cannot predict if investors will find our common stock less attractive because we will rely on these exemptions. If some investors find our common stock less attractive as a result, there may be a less active trading market for
58
Table of Contents
our common stock and our stock price may be more volatile. We may take advantage of these reporting exemptions until we are no longer an emerging growth company. We will remain an emerging growth company until the earlier of (1) the last day of the fiscal year (a) following the fifth anniversary of the completion of this offering, (b) in which we have total annual gross revenue of at least $1.07 billion, or (c) in which we are deemed to be a large accelerated filer, which means the market value of our common stock that is held by non-affiliates exceeds $700 million as of the prior June 30, and (2) the date on which we have issued more than $1.0 billion in non-convertible debt during the prior three-year period.
If we are unable to implement and maintain effective internal control over financial reporting in the future, investors may lose confidence in the accuracy and completeness of our financial reports and the market price of our common stock could be adversely affected.
As a public company, we will be required to maintain internal control over financial reporting and to report any material weaknesses in such internal control. Section 404 of the Sarbanes-Oxley Act requires that we evaluate and determine the effectiveness of our internal control over financial reporting and, beginning with our second annual report following this offering, which will be for our fiscal year ending December 31, 2019, provide a management report on internal control over financial reporting. The Sarbanes-Oxley Act also requires that our management report on internal control over financial reporting be attested to by our independent registered public accounting firm, to the extent we are no longer an “emerging growth company,” as defined by the JOBS Act. We do not expect to have our independent registered public accounting firm attest to our management report on internal control over financial reporting for so long as we are an emerging growth company.
If we have a material weakness in our internal control over financial reporting, we may not detect errors on a timely basis and our financial statements may be materially misstated. We are in the process of designing and implementing the internal control over financial reporting required to comply with this obligation, which process will be time consuming, costly and complicated. If we identify material weaknesses in our internal control over financial reporting, if we are unable to comply with the requirements of Section 404 in a timely manner, if we are unable to assert that our internal control over financial reporting is effective, or, when required in the future, if our independent registered public accounting firm is unable to express an opinion as to the effectiveness of our internal control over financial reporting, investors may lose confidence in the accuracy and completeness of our financial reports and the market price of our common stock could be adversely affected, and we could become subject to investigations by the stock exchange on which our securities are listed, the SEC, or other regulatory authorities, which could require additional financial and management resources.
Purchasers in this offering will experience immediate and substantial dilution in the book value of their investment.
The initial public offering price of our common stock is substantially higher than the net tangible book value per share of our common stock immediately after this offering. Accordingly, if you purchase our common stock in this offering, you will incur immediate substantial dilution of approximately $ per share, based on the initial public offering price of $ per share. In addition, following this offering, purchasers in this offering will have contributed approximately of the total gross consideration paid by stockholders to us to purchase shares of our common stock, but will own only approximately of the shares of common stock outstanding immediately after this offering. Furthermore, if the underwriters exercise their option to purchase additional shares, outstanding options or convertible securities are exercised, or we sell shares of our common stock in future financings, you could experience further dilution. For a further description of the dilution that you will experience immediately after this offering, see the section titled “Dilution.”
59
Table of Contents
Sales of a substantial number of shares of our common stock in the public market could cause our stock price to fall.
If our existing stockholders sell, or indicate an intention to sell, substantial amounts of our common stock in the public market after the lock-up and other legal restrictions on resale discussed in this prospectus lapse, the trading price of our common stock could decline. Based upon the number of shares outstanding as of , 2018, upon the closing of this offering, we will have outstanding a total of approximately million shares of common stock, assuming no exercise of the underwriters’ option to purchase additional shares. Of these shares, shares of our common stock, plus any shares sold upon exercise of the underwriters’ option to purchase additional shares, will be freely tradable, without restriction, in the public market immediately following this offering. Piper Jaffray & Co., however, may, in its/their sole discretion, permit our officers, directors and other stockholders who are subject to lock-up agreements to sell shares prior to the expiration of the lock-up agreements.
The lock-up agreements pertaining to this offering will expire 180 days from the date of this prospectus. After the lock-up agreements expire, up to an additional approximately million shares of common stock will be eligible for sale in the public market, approximately million of which are held by current directors, executive officers and other affiliates and may be subject to Rule 144 under the Securities Act of 1933, as amended, or the Securities Act.
In addition, as of , 2018, approximately million shares of common stock that are subject to outstanding options will become eligible for sale in the public market to the extent permitted by the provisions of various vesting schedules, the lock-up agreements and Rule 144 and Rule 701 under the Securities Act. If these additional shares of common stock are sold, or if it is perceived that they will be sold, in the public market, the trading price of our common stock could decline.
After this offering, the holders of approximately million shares of our outstanding common stock, including shares issuable upon exercise of outstanding options, will be entitled to rights with respect to the registration of their shares under the Securities Act, subject to vesting schedules and to the lock-up agreements described above. Registration of these shares under the Securities Act would result in the shares becoming freely tradable without restriction under the Securities Act, except for shares purchased by affiliates. Any sales of securities by these stockholders could have a material adverse effect on the trading price of our common stock.
Our principal stockholders and management own a significant percentage of our stock and will be able to exert significant control over matters subject to stockholder approval.
As of , 2018, our executive officers, directors, holders of 5% or more of our capital stock and their respective affiliates beneficially owned approximately of our outstanding voting stock and, upon the closing of this offering, that same group will beneficially own approximately of our outstanding voting stock (assuming no exercise of the underwriters’ option to purchase additional shares and no exercise of outstanding options). Therefore, even after this offering these stockholders will have the ability to influence us through this ownership position. These stockholders may be able to determine all matters requiring stockholder approval. For example, these stockholders may be able to control elections of directors, amendments of our organizational documents, or approval of any merger, sale of assets, or other major corporate transaction. This may prevent or discourage unsolicited acquisition proposals or offers for our common stock that you may feel are in your best interest as one of our stockholders.
60
Table of Contents
Provisions in our charter documents and under Delaware law could discourage a takeover that stockholders may consider favorable and may lead to entrenchment of management.
Our certificate of incorporation and bylaws that will be in effect prior to the consummation of this offering will contain provisions that could significantly reduce the value of our shares to a potential acquirer or delay or prevent changes in control or changes in our management without the consent of our board of directors. The provisions in our charter documents will include the following:
| • | a classified board of directors with three-year staggered terms, which may delay the ability of stockholders to change the membership of a majority of our board of directors; |
| • | cumulative voting in the election of directors, which limits the ability of minority stockholders to elect director candidates; |
| • | the exclusive right of our board of directors to elect a director to fill a vacancy created by the expansion of the board of directors or the resignation, death or removal of a director, which prevents stockholders from being able to fill vacancies on our board of directors; |
| • | the required approval of at least 66 2/3% of the shares entitled to vote to remove a director for cause, and the prohibition on removal of directors without cause; |
| • | the ability of our board of directors to authorize the issuance of shares of preferred stock and to determine the price and other terms of those shares, including preferences and voting rights, without stockholder approval, which could be used to significantly dilute the ownership of a hostile acquiror; |
| • | the ability of our board of directors to alter our bylaws without obtaining stockholder approval; |
| • | the required approval of at least 66 2/3% of the shares entitled to vote at an election of directors to adopt, amend or repeal our bylaws or repeal the provisions of our amended and restated certificate of incorporation regarding the election and removal of directors; |
| • | a prohibition on stockholder action by written consent, which forces stockholder action to be taken at an annual or special meeting of our stockholders; |
| • | the requirement that a special meeting of stockholders may be called only by the chairman of the board of directors, the chief executive officer, the president or the board of directors, which may delay the ability of our stockholders to force consideration of a proposal or to take action, including the removal of directors; and |
| • | advance notice procedures that stockholders must comply with in order to nominate candidates to our board of directors or to propose matters to be acted upon at a stockholders’ meeting, which may discourage or deter a potential acquiror from conducting a solicitation of proxies to elect the acquiror’s own slate of directors or otherwise attempting to obtain control of us. |
In addition, these provisions would apply even if we were to receive an offer that some stockholders may consider beneficial.
We are also subject to the anti-takeover provisions contained in Section 203 of the Delaware General Corporation Law. Under Section 203, a corporation may not, in general, engage in a business combination with any holder of 15% or more of its capital stock unless the holder has held the stock for three years or, among other exceptions, the board of directors has approved the transaction. For a description of our capital stock, see the section titled “Description of Capital Stock.”
61
Table of Contents
Claims for indemnification by our directors and officers may reduce our available funds to satisfy successful third-party claims against us and may reduce the amount of money available to us.
Our certificate of incorporation and bylaws provide that we will indemnify our directors and officers to the fullest extent permitted by Delaware law.
In addition, as permitted by Section 145 of the Delaware General Corporation Law, or the DGCL, our amended and restated bylaws to be effective immediately prior to the completion of this offering and our indemnification agreements that we have entered into with our directors and officers provide that:
| • | we will indemnify our directors and officers for serving us in those capacities or for serving other business enterprises at our request, to the fullest extent permitted by Delaware law. Delaware law provides that a corporation may indemnify such person if such person acted in good faith and in a manner such person reasonably believed to be in or not opposed to the best interests of the registrant and, with respect to any criminal proceeding, had no reasonable cause to believe such person’s conduct was unlawful; |
| • | we may, in our discretion, indemnify employees and agents in those circumstances where indemnification is permitted by applicable law; |
| • | we are required to advance expenses, as incurred, to our directors and officers in connection with defending a proceeding, except that such directors or officers shall undertake to repay such advances if it is ultimately determined that such person is not entitled to indemnification; |
| • | we will not be obligated pursuant to our amended and restated bylaws to indemnify a person with respect to proceedings initiated by that person against us or our other indemnitees, except with respect to proceedings authorized by our board of directors or brought to enforce a right to indemnification; |
| • | the rights conferred in our amended and restated bylaws are not exclusive, and we are authorized to enter into indemnification agreements with our directors, officers, employees and agents and to obtain insurance to indemnify such persons; and |
| • | we may not retroactively amend our amended and restated bylaw provisions to reduce our indemnification obligations to directors, officers, employees and agents. |
We do not currently intend to pay dividends on our common stock, and, consequently, your ability to achieve a return on your investment will depend on appreciation in the price of our common stock.
We do not currently intend to pay any cash dividends on our common stock for the foreseeable future. We currently intend to invest our future earnings, if any, to fund our growth. Therefore, you are not likely to receive any dividends on your common stock for the foreseeable future. Since we do not intend to pay dividends, your ability to receive a return on your investment will depend on any future appreciation in the market value of our common stock. There is no guarantee that our common stock will appreciate or even maintain the price at which our holders have purchased it.
Comprehensive U.S. federal income tax reform could adversely affect us.
On December 22, 2017, President Trump signed into law the “Tax Cuts and Jobs Act”, or TCJA, that significantly reforms the Internal Revenue Code of 1986, or the Code, as amended. The TCJA, among other things, includes changes to U.S. federal tax rates, imposes significant additional limitations on the deductibility of interest, allows for the expensing of capital expenditures, and puts into effect the migration from a “worldwide” system of taxation to a modified territorial system. We continue to examine the impact this tax reform legislation may have on our business. The impact of this tax reform on holders of our common stock is uncertain and could be adverse. This prospectus does not discuss any such tax legislation or the manner in which it might affect purchasers of our common stock. We urge our stockholders, including purchasers of common stock in this offering, to consult with their legal and tax advisors with respect to such legislation and the potential tax consequences of investing in our common stock.
62
Table of Contents
SPECIAL NOTE REGARDING FORWARD-LOOKING STATEMENTS
This prospectus contains statements that express our opinions, expectations, beliefs, plans, objectives, assumptions or projections regarding future events or future results, in contrast with statements that reflect historical facts. Many of these statements are contained under the headings “Prospectus Summary,” “Management’s Discussion and Analysis of Financial Condition and Results of Operations” and “Business.” In some cases, we have identified such forward-looking statements with typical conditional words such as “anticipate,” “intend,” “believe,” “estimate,” “plan,” “seek,” “project,” “expect,” “may,” “will,” “would,” “could,” “should,” the negative of these terms or other comparable terminology.
Forward-looking statements are not a guarantee of performance, and you should not place undue reliance on such statements. We have based forward-looking statements largely on our current expectations and projections about future events. Forward-looking statements are subject to many uncertainties and other variable circumstances, including those discussed in this prospectus under the headings “Risk Factors” and “Management’s Discussion and Analysis of Financial Condition and Results of Operations,” many of which are outside of our control, that could cause our actual results and experience to differ materially from any forward-looking statement. Given these risks and uncertainties, you are cautioned not to place undue reliance on these forward-looking statements. The forward-looking statements included in this prospectus are made only as of the date hereof. We do not undertake, and specifically decline, any obligation to update any such statements or to publicly announce the results of any revisions to any of such statements to reflect future events or developments.
63
Table of Contents
We estimate, based upon an assumed initial public offering price of $ per share, which is the midpoint of the price range set forth on the cover page of this prospectus, we will receive net proceeds from this offering of approximately $ million (or $ million if the underwriters exercise their option to purchase additional shares in full), after deducting estimated underwriting discounts and commissions and estimated offering expenses payable by us.
The principal purposes of this offering are to obtain additional capital to support our operations, create a public market for our common stock and to facilitate future access to the public equity markets. We currently estimate that we will use the net proceeds from this offering for working capital and other corporate purposes including to (i) continue funding our activities related to the commercial launch of gammaCore, initially for the acute treatment of migraine and episodic cluster headache in the United States, (ii) invest in the expansion of gammaCore into additional indications in headache and rheumatology, and (iii) further build out our specialty distribution channel for gammaCore Sapphire.
In addition, we may also use a portion of our net proceeds to acquire and invest in complementary products, technologies, services or businesses; however, we currently have no plans, agreements or commitments to complete any such transaction nor are we involved in negotiations to do so.
Our expected use of net proceeds from this offering represents our current intentions based upon our plans and business condition. As of the date of this prospectus, we cannot predict with certainty all of the particular uses for the net proceeds to be received upon the completion of this offering or the amounts that we will actually spend on the uses set forth above. The amounts and timing of our actual use of the net proceeds will vary depending on numerous factors, including the factors described under the heading “Risk Factors” in this prospectus. As a result, management will have broad discretion in its application of the net proceeds, and investors will be relying on our judgment in such application.
Pending use of the net proceeds from this offering, we may invest in short- and intermediate-term interest-bearing obligations, investment-grade instruments, certificates of deposit or direct or guaranteed obligations of the U.S. government.
Although it is difficult to predict future liquidity requirements, we believe that the net proceeds from this offering, together with our existing cash and cash equivalents, will be sufficient to fund our operations for at least the next twelve months.
64
Table of Contents
We have never declared or paid cash dividends on our capital stock. We do not expect to pay dividends on our common stock for the foreseeable future. Instead, we anticipate that all of our earnings, if any, will be used for the operation and growth of our business. Any future determination to declare cash dividends would be subject to the discretion of our board of directors and would depend upon various factors, including our results of operations, financial condition and capital requirements, restrictions that may be imposed by applicable law and our contracts and other factors deemed relevant by our board of directors.
65
Table of Contents
We currently operate as a Delaware limited liability company under the name Electrocore, LLC. Prior to the closing of this offering, Electrocore, LLC will convert into a Delaware corporation pursuant to a statutory conversion and change its name to electroCore, Inc. In order to consummate the corporate conversion, a certificate of conversion will be filed with the Secretary of State of the State of Delaware. As part of the corporate conversion, based on the assumed initial public offering price of $ per share, which is the midpoint of the price range set forth on the cover page of this prospectus, all Units will be converted into an aggregate of shares of our common stock and options to purchase shares of our common stock as follows:
| • | holders of our common units, or Common Units, other than Common Units that were originally issued as “profits interests” (as such term is used for purposes of the Code), or Profits Interests, will receive an aggregate of shares of our common stock; |
| • | holders of our Series A Preferred Units will receive an aggregate of shares of our common stock, which includes shares of our common stock as payment in full of the accrued and unpaid preference payable in respect of the Series A Preferred Units; |
| • | holders of our Series B Preferred Units will receive an aggregate of shares of our common stock; and |
| • | holders of our Profits Interests will receive an aggregate of shares of our common stock and, with respect to such holders who are our employees or consultants at the time of the corporate conversion, options to purchase an aggregate of shares of our common stock, with an exercise price equal to the initial public offering price. |
In addition, based on the assumed initial public offering price of $ per share, which is the midpoint of the price range set forth on the cover page of this prospectus:
| • | warrants, other than warrants that expire in connection with this offering, to purchase Common Units will be converted into warrants to purchase shares of our common stock; |
| • | warrants to purchase Series A Preferred Units will be converted into warrants to purchase shares of our common stock; and |
| • | warrants to purchase Series B Preferred Units will be converted into warrants to purchase shares of our common stock. |
The number of shares of common stock and the number of shares of common stock issuable pursuant to options and warrants in connection with the corporate conversion will be determined pursuant to the applicable provisions of the plan of conversion, which is based upon terms of our Operating Agreement. The Operating Agreement provides that each outstanding series of our Preferred Units will automatically convert (which we refer to as the Automatic Conversion) into Common Units at the applicable conversion ratio (currently, on a one-for-one basis) upon either the closing of a Qualified Public Offering, as defined in the Operating Agreement, or the written consent executed by members of Electrocore, LLC holding a sufficient number of each class of our Preferred Units and Common Units as required under our Operating Agreement. We anticipate receiving written consents from the required holders of our Units to effect the Automatic Conversion.
Following the Automatic Conversion and effective upon the consummation of the corporate conversion, all of the outstanding Units will convert into a number of shares of common stock and options to purchase common stock of electroCore, Inc. based upon the value of Electrocore, LLC at the time of this offering with a value implied by the initial public offering price of the shares of common stock sold in
66
Table of Contents
this offering. Upon conversion, the shares of common stock of electroCore, Inc. and options to purchase our common stock will be allocated among the various classes and series of Units in accordance with the distribution and other applicable provisions set forth in the Operating Agreement. Similarly, the number of shares of common stock for which warrants will become exercisable following the corporate conversion will be determined based on the terms of such warrants. No cash or fractional shares of common stock will be issued in connection with the corporate conversion.
In connection with the corporate conversion, all outstanding Common Units, other than Common Units issued as Profits Interests, and Preferred Units of Electrocore, LLC will be converted into our common stock on a one-for-one basis. In addition, we expect to issue shares of our common stock to the holders of our Series A Preferred Units to satisfy approximately $3.6 million of accrued and unpaid preference return on such units. Additionally, in connection with the corporate conversion, our Profits Interests will be converted into (i) shares of our common stock, and (ii) with respect to Profits Interests that are held by our current employees and consultants at the time of the conversion, options to purchase our common stock. The number of shares of common stock and the number of options to be issued to each such holder of Profits Interests will be determined based upon the appreciation in our value after the date of grant of the applicable Profits Interests through the completion of this offering. The exercise price of these options will be equal to the initial public offering price. Following the corporate conversion, the vesting provisions applicable to the Profits Interests as in effect prior to the corporate conversion will apply, in substantially the same manner, to the shares of common stock and options issued in respect of such Profits Interests in the corporate conversion.
Because the exact number of shares of our common stock to be issued to holders of Units in the corporate conversion, the number of shares of common stock for which warrants will be exercisable following the corporate conversion and the number of shares of common stock and options to purchase common stock that holders of Profits Interests will receive in the corporate conversion is based on the initial public offering price, to the extent that the actual initial public offering price per share for this offering is greater or less than $ , which is the midpoint of the price range set forth on the cover page of this prospectus, the actual number of shares of common stock to be issued to holders of Units, the number of shares of common stock for which options and warrants will be exercisable and the total number of shares of common stock outstanding following the corporate conversion will be adjusted accordingly.
In connection with the corporate conversion, electroCore, Inc. will hold all property and assets of Electrocore, LLC and all of the debts and obligations of Electrocore, LLC will become the debts and obligations of electroCore, Inc. by operation of law. electroCore, Inc. will be governed by a certificate of incorporation filed with the Delaware Secretary of State and bylaws, the material portions of each of which are described under the heading “Description of Capital Stock.”
On the effective date of the corporate conversion, the members of the board of managers of Electrocore, LLC will become the members of electroCore, Inc.’s board of directors and the officers of Electrocore, LLC will become the officers of electroCore, Inc.
The purpose of the corporate conversion is to reorganize our corporate structure so that the entity that is offering common stock to the public in this offering is a corporation rather than a limited liability company and so that our existing investors will own our common stock rather than equity interests in a limited liability company. References in this prospectus to our capitalization and other matters pertaining to our equity and shares prior to the corporate conversion relate to the capitalization and equity and units of Electrocore, LLC, and after the corporate conversion, to electroCore, Inc.
The audited consolidated financial statements included elsewhere in this prospectus are those of Electrocore, LLC and its subsidiaries and affiliate. We expect that our conversion from a Delaware limited liability company to a Delaware corporation will not have a material effect on our audited consolidated financial statements at the time of the corporate conversion.
67
Table of Contents
The following table sets forth our cash, cash equivalents and short-term investments and our capitalization as of December 31, 2017:
| • | on an actual basis; |
| • | on a pro forma basis to give effect to the corporate conversion, based on the assumed initial public offering price of $ per share, which is the midpoint of the price range set forth on the cover page of this prospectus; and |
| • | on a pro forma as adjusted basis to give further effect to the sale of shares of our common stock in this offering, assuming an initial public offering price of $ per share, which is the midpoint of the price range set forth on the cover page of this prospectus, after deducting estimated underwriting discounts and commissions and estimated offering expenses payable by us and the application of the proceeds therefrom. |
The pro forma and pro forma as adjusted information below is illustrative only, and our capitalization following the corporate conversion and the closing of this offering will depend on the actual initial public offering price and other terms of this offering determined at pricing. You should read the following information together with the information contained under the headings “Selected Consolidated Financial Data” and “Management’s Discussion and Analysis of Financial Condition and Results of Operations” and our audited consolidated financial statements and the accompanying notes appearing elsewhere in this prospectus.
| As of December 31, 2017 | ||||||||||||
| Actual | Pro forma(2)(3)(4) | Pro forma as adjusted(1)(4) |
||||||||||
| (unaudited; in thousands, except unit and share data) | ||||||||||||
| Cash, cash equivalents and short-term investments |
$ | $ | $ | |||||||||
|
|
|
|
|
|
|
|||||||
| Warrant liability |
$ | $ | $ | |||||||||
|
|
|
|
|
|
|
|||||||
| Members’/stockholders’ equity (deficit): |
||||||||||||
| Common units, units
authorized; |
||||||||||||
| Common stock, par value $ per share; shares authorized; shares issued and outstanding, pro forma; shares issued and outstanding, pro forma as adjusted |
||||||||||||
| Series A Preferred Units, 70,918,506 units issued and outstanding |
||||||||||||
| Series B Preferred Units, 105,150,162 units issued and outstanding |
||||||||||||
| Additional paid-in capital |
||||||||||||
| Accumulated deficit |
||||||||||||
|
|
|
|
|
|
|
|||||||
| Total members’/stockholders’ equity (deficit) |
||||||||||||
|
|
|
|
|
|
|
|||||||
| Total capitalization |
$ | $ | $ | |||||||||
|
|
|
|
|
|
|
|||||||
68
Table of Contents
| (1) | Each $1.00 increase (decrease) in the assumed initial public offering price of $ per share, which is the midpoint of the price range set forth on the cover page of this prospectus, would increase (decrease) the pro forma as adjusted amount of each of cash and cash equivalents and short term investments, additional paid in capital, total stockholders’ equity and total capitalization by $ million, assuming that the number of shares offered by us, as set forth on the cover page of this prospectus, remains the same and after deducting the estimated underwriting discounts and commissions and estimated offering expenses payable by us. Similarly, each increase (decrease) of 1.0 million shares in the number of shares offered by us at the assumed initial public offering price per share, which is the midpoint of the price range set forth on the cover page of this prospectus, would increase (decrease) the pro forma as adjusted amount of each of cash and cash equivalents and short term investments, additional paid in capital, total stockholders’ equity and total capitalization by $ million. |
| (2) | In connection with the corporate conversion, Common Units, Series A Preferred Units, Series B Preferred Units, additional paid-in capital and accumulated deficit will be reduced to zero to reflect the elimination of all outstanding Units and other interests in Electrocore, LLC and corresponding adjustments will be reflected as common stock, additional paid-in capital, and total stockholders’ equity (deficit). |
| (3) | The following table presents the number of shares of common stock issuable in connection with the corporate conversion to holders of Series A Preferred Units, Series B Preferred Units, and Common Units, based on the assumed initial public offering price per common share of $ , which is the midpoint of the price range set forth on the cover page of this prospectus. |
| Common stock issuable for: |
||||
| Common Units |
||||
| Series A Preferred Units |
||||
| Series B Preferred Units |
||||
| Profits Interests |
||||
| Total |
||||
|
|
|
| (4) | The pro forma and pro forma as adjusted information discussed above are illustrative only. |
The capitalization table presented above excludes, after giving effect to the corporate conversion:
| • | shares of common stock issuable upon exercise of outstanding options or options to be issued for certain profits interests to purchase shares of common stock as of , at a weighted-average exercise price equal to the assumed initial public offering price per share of common stock of $ , which is the midpoint of the price range set forth on the cover page of this prospectus; and |
| • | an additional shares of common stock reserved for future issuance under the 2018 Plan; and |
| • | shares issuable upon the exercise of warrants at a weighted-average exercise price of $ per share following the corporate conversion. |
69
Table of Contents
If you invest in our common stock, your ownership interest will be diluted immediately to the extent of the difference between the initial public offering price per share of our common stock and the pro forma as adjusted net tangible book value per share of our common stock immediately after this offering. Net tangible book value per share represents the book value of our total tangible assets less the book value of our total liabilities divided by the number of shares of common stock then issued and outstanding.
After giving effect to the corporate conversion, pro forma net tangible book value as of December 31, 2017 was $ million, or $ per share based on the shares of common stock issued and outstanding after the corporate conversion based on an assumed initial public offering price of $ per share (the midpoint of the price range set forth on the cover page of this prospectus). After giving effect to our sale of common stock in this offering at the initial public offering price of $ per share (the midpoint of the price range set forth on the cover page of this prospectus), and after deducting estimated underwriting discounts and commissions and estimated offering expenses payable by us, our pro forma as adjusted net tangible book value as of December 31, 2017 would have been $ million, or $ per share (assuming no exercise of the underwriters’ option to purchase additional shares of our common stock). This represents an immediate and substantial dilution of $ per share to new investors purchasing common stock in this offering. The following table illustrates this dilution per share:
| Assumed initial public offering price per share |
$ | |||||||
| Pro forma net tangible book value per share as of December 31, 2017 |
$ | |||||||
| Decrease in net tangible book value per share attributable to this offering |
$ | |||||||
|
|
|
|||||||
| Pro forma as adjusted net tangible book value per share after giving effect to this offering |
$ | |||||||
|
|
|
|||||||
| Dilution per share to new investors in this offering |
$ | |||||||
|
|
|
If the underwriters exercise their option to purchase additional shares in full, our pro forma as adjusted net tangible book value per share after this offering would be $ per share, and the dilution in pro forma net tangible book value per share to new investors in this offering would be $ per share.
The following table summarizes, on a pro forma as adjusted basis as of December 31, 2017, the differences between the number of shares of common stock purchased from us, the total price and the average price per share paid by existing stockholders and by the new investors in this offering, before deducting estimated underwriting discounts and commissions and estimated offering expenses payable by us, at an assumed initial public offering price of $ per share (the midpoint of the price range set forth on the cover page of this prospectus).
| Shares purchased | Total consideration | Average price per share |
||||||||||||||||||
| Number | Percent | Amount | Percent | |||||||||||||||||
| (in millions) | ||||||||||||||||||||
| Existing investors |
% | $ | % | $ | ||||||||||||||||
| New investors in this offering |
$ | |||||||||||||||||||
| Total |
% | $ | % | $ | ||||||||||||||||
70
Table of Contents
The discussion and table above assume no exercise of stock options to be outstanding after giving effect to the corporate conversion and no issuance of shares of our common stock reserved for issuance under our 2018 Plan, which include:
| • | shares issuable upon the exercise of options to be outstanding after giving effect to the corporate conversion at an exercise price equal to the initial public offering price of $ per share following the corporate conversion; |
| • | shares issuable upon the exercise of warrants at a weighted-average exercise price of $ per share following the corporate conversion; and |
| • | shares of common stock reserved for issuance pursuant to future awards under the 2018 Plan, which will become effective immediately prior to the consummation of this offering. |
If, after giving effect to the corporate conversion, all of our outstanding options to be outstanding after giving effect to the corporate conversion and warrants were exercised, our pro forma as adjusted net tangible book value as of December 31, 2017 would have been $ per share and our pro forma as adjusted net tangible book value after giving effect to this offering would have been $ per share, causing dilution to new investors purchasing shares in this offering of $ per share. Shares purchased by new investors would then represent % of the shares purchased from us for % of the total consideration.
To the extent that options to be outstanding after giving effect to the corporate conversion are exercised, new options are issued under the 2018 Plan, or we issue additional shares of common stock in the future, there will be further dilution to investors participating in this offering. In addition, we may choose to raise additional capital because of market conditions or strategic considerations, even if we believe that we have sufficient funds for our current or future operating plans. If we raise additional capital through the sale of equity or convertible debt securities, the issuance of these securities could result in further dilution to our stockholders.
The number of shares of common stock of electroCore, Inc. that holders of units will receive in the corporate conversion and the number of shares of common stock that options and warrants will be exercisable for following the corporate conversion will vary depending on the initial public offering price set forth on the cover page of this prospectus.
71
Table of Contents
SELECTED CONSOLIDATED FINANCIAL DATA
The selected consolidated statements of operations data for the years ended December 31, 2016 and 2017 and the selected consolidated balance sheet data as of December 31, 2016 and 2017 are derived from our audited consolidated financial statements included elsewhere in this prospectus. Our historical results are not necessarily indicative of the results that may be expected in any future period. The selected consolidated financial data below should be read in conjunction with the section entitled “Management’s Discussion and Analysis of Financial Condition and Results of Operations” and our audited consolidated financial statements and related notes included elsewhere in this prospectus.
| Year ended December 31, | ||||||||
| 2016 | 2017 | |||||||
| |
(in thousands; except for unit and per unit amounts) |
| ||||||
| Consolidated statements of operations: |
||||||||
| Net sales |
$ | 254.1 | ||||||
| Cost of goods sold |
123.7 | |||||||
|
|
|
|
|
|||||
| Gross profit |
130.4 | |||||||
| Operating expenses |
||||||||
| Research and development |
7,971.3 | |||||||
| Selling, general and administrative |
7,169.3 | |||||||
|
|
|
|
|
|||||
| Total operating expenses |
15,140.6 | |||||||
|
|
|
|
|
|||||
| Loss from operations |
(15,010.2 | ) | ||||||
| Amortization of debt discount and issuance costs |
536.9 | |||||||
| Interest expense |
234.4 | |||||||
|
|
|
|
|
|||||
| Net loss |
(15,781.5 | ) | ||||||
| Less net loss attributable to noncontrolling interest |
(44.1 | ) | ||||||
|
|
|
|
|
|||||
| Net loss attributable to Electrocore, LLC, subsidiaries and affiliates |
$ | (15,737.4 | ) | |||||
|
|
|
|
|
|||||
| Pro forma net loss per unit data(1): |
||||||||
| Pro forma net loss per unit—basic and diluted (unaudited) |
$ | (0.10 | ) | |||||
| Pro forma weighted average number of common units used to calculate loss per unit—basic and diluted (unaudited) |
150,566,206 | |||||||
| As of December 31, | ||||||||
| 2016 | 2017 | |||||||
| (in thousands) | ||||||||
| Consolidated balance sheet data: |
||||||||
| Cash and cash equivalents |
$ | 416.3 | ||||||
| Working capital(2) |
(3,629.4 | ) | ||||||
| Total assets |
622.0 | |||||||
| Long-term debt |
3,665.9 | |||||||
| Series A Preferred Units |
53,518.5 | |||||||
| Series B Preferred Units |
— | |||||||
| Common Units |
30,912.1 | |||||||
| Total members’ equity (deficit) |
$ | (7,535.0 | ) | |||||
| (1) | We have presented pro forma basic and diluted net loss per unit for the year ended December 31, 2016, which consists of our historical net loss attributable to Electrocore LLC, subsidiaries and affiliate, divided by the pro forma basic and diluted weighted average number of units of common stock outstanding after giving effect to the conversion of all of our outstanding Series A Preferred Units into |
72
Table of Contents
| 70,918,506 shares of our common stock prior to the closing of this offering. We have presented pro forma basic and diluted net loss per unit for the year ended December 31, 2017, which consists of our historical net loss attributable to Electrocore LLC, subsidiaries and affiliate, divided by the pro forma basic and diluted weighted average number of units of common stock outstanding after giving effect to the conversion of all of our outstanding Series A Preferred Units and Series B Preferred Units into shares of our common stock prior to the closing of this offering. Net loss used in calculating net loss per unit does not reflect the (i) estimated expenses of this offering or (ii) compensation and expenses for our board of directors and other costs related to operating as a public company. For more information on how we calculate basic and diluted pro forma weighted average number of shares outstanding, see Note 8 to our audited consolidated financial statements included elsewhere in this prospectus. The calculations described above do not give effect to the potential issuance of shares of common stock at the initial public offering price in satisfaction of accrued but unpaid preference to our preferred stockholders (which may be paid in cash or such shares, at our option). |
| (2) | We define working capital as current assets less current liabilities. |
73
Table of Contents
MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL
CONDITION AND RESULTS OF OPERATIONS
The following discussion of our results of operations and financial condition should be read together with the audited historical financial statements and the notes therein included in this prospectus as well as the discussion in the Business section of this prospectus. This discussion contains forward-looking statements that involve risks and uncertainties. The forward-looking statements are not historical facts, but rather are based on current expectations, estimates, assumptions and projections about our industry, business and future financial results. Our actual results could differ materially from the results contemplated by these forward-looking statements due to a number of factors, including those discussed in the sections of this prospectus entitled “Risk Factors” and “Special Note Regarding Forward-Looking Statements.”
Overview
We are a commercial-stage bioelectronic medicine company with a platform non-invasive vagus nerve stimulation therapy initially focused on neurology and rheumatology. Our therapy, gammaCore, has pharmacologic effects on the peripheral and central nervous systems, which modulate neurotransmitters and immune function. gammaCore is FDA-cleared for the acute treatment of pain associated with migraine and episodic cluster headache. Based on our clinical data, we are pursuing label expansions for the prevention of migraine, migraine in adolescents and post-traumatic headache, and are also engaging in clinical development for potential new labeling claims in rheumatology, including Sjôgren’s syndrome and rheumatoid arthritis.
Following our initial FDA clearance, our commercial strategy has been to establish gammaCore as a first-line treatment option for episodic cluster headache patients, who have few alternative treatment options available to them. This strategy is supported by a product registry initiated in July 2017 to build advocacy among key opinion leaders in 55 leading headache centers in the United States, and to generate patient demand in the form of prescriptions submitted to payors. We intend to leverage this advocacy as we expand into the broader headache market for both migraine and cluster headache in the second quarter of 2018.
Since our inception in 2005, we have devoted substantially all of our resources to the development of vagus nerve stimulation, or VNS, and the commercialization of our gammaCore therapy. Since our inception, we have received gross cash proceeds of approximately $160.3 million from the sale of our equity securities, including the conversion or exercise of our convertible promissory notes, term loan and warrants. In 2017, in connection with closings of our Series B Preferred Unit financing, we received net cash proceeds of approximately $ million net of the conversion of outstanding bridge notes and accrued interest thereon.
We have never been profitable and have incurred net losses in each year since our inception. We incurred net losses of $ million and $15.7 million for the years ended December 31, 2017 and 2016, respectively. As of December 31, 2017, our accumulated deficit was $ million. We expect to continue to incur substantial net losses and negative cash flows from operations for at least the next several years as we commercialize gammaCore for the acute treatment of pain associated with migraine and episodic cluster headache in adults. We intend to make a significant investment in building our U.S. commercial infrastructure and in recruiting and training our sales representatives. We also intend to continue to make significant investments in research and development to expand our gammaCore therapy for the treatment of other indications, including additional headache conditions and rheumatology. Furthermore, upon the closing of this offering, we expect to incur additional costs associated with operating as a public company, including significant legal, accounting, investor relations and other expenses that we did not incur as a private company.
74
Table of Contents
As a result, we will need substantial additional funding to support our continuing operations and pursue our growth strategy. Until such time as we can generate sufficient revenue to cover our operating expenses and growth strategy, if ever, we expect to finance our operations through the sale of equity, debt financings or other capital sources, including potential collaborations with other companies and other strategic transactions. We may be unable to raise additional funds or enter into such other agreements or arrangements when needed on favorable terms, or at all. If we fail to raise capital or enter into such agreements as, and when needed, we may have to significantly delay, scale back or discontinue the development and commercialization of gammaCore, or delay our pursuit of potential additional labeling claims.
We face a variety of challenges and risks, which we will need to address and manage as we pursue our strategy, including our ability to develop and retain an effective sales force, achieve market acceptance of gammaCore among physicians, patients and third-party payors, and expand the use of gammaCore to additional therapeutic indications.
Because of the numerous risks and uncertainties associated with our commercialization efforts, as well as research and clinical development activities, we are unable to predict the timing or amount of increased expenses, or when, if ever, we will be able to achieve or maintain profitability. Even if we are able to increase sales of gammaCore, we may not become profitable. If we fail to become profitable or are unable to sustain profitability, then we may be unable to continue our operations at planned levels and be forced to reduce or terminate our operations.
As of December 31, 2017, we had cash and cash equivalents, and short-term investments, of $ million. We believe that the anticipated net proceeds from this offering, together with our existing cash resources, will enable us to fund our operating expenses and capital expenditure requirements through at least the next 12 months. We have based these estimates on assumptions that may prove to be wrong, and we could exhaust our available capital resources sooner than we expect. See “—Liquidity and Capital Resources.”
Statutory Corporate Conversion
We currently operate as a Delaware limited liability company, under the name Electrocore, LLC. Prior to the closing of this offering, Electrocore, LLC will convert into a Delaware corporation pursuant to a statutory conversion and change its name to electroCore, Inc. As a result of the corporate conversion, the holders of the different classes and series of units of Electrocore, LLC will become holders of common stock and options to purchase common stock of electroCore, Inc. Our Common Units, other than Common Units issued as profits interest under the Code, or Profits Interests, Series A Preferred Units and Series B Preferred Units will convert into shares of our common stock on a one-for-one basis in the corporate conversion. Our Profits Interest will be converted into (i) shares of our common stock, and (ii) with respect to Profits Interests that are held by our current employees and consultants at the time of the corporate conversion, options to purchase our common stock. The number of shares of common stock and the number of options to be issued in respect of the Profits Interests will be determined based upon the appreciation in our value after the date of grant of the applicable Profits Interest through the completion of this offering. The exercise price of these options will be equal to our initial public offering price. Following the corporate conversion, the vesting provisions applicable to the Profits Interests as in effect prior to the corporate conversion will apply, in substantially the same manner, to the shares of common stock and options issued in respect of such Profits Interests in the corporate conversion. Other than warrants that expire in connection with the completion of this offering, holders of warrants to purchase units of ElectroCore, LLC will become holders of warrants to purchase common stock of electroCore, Inc.
The purpose of the corporate conversion is to reorganize our corporate structure so that the entity that is offering our common stock to the public in this offering is a corporation rather than a limited liability
75
Table of Contents
company and so that our existing investors will own our common stock rather than equity interests in a limited liability company. For further information regarding the corporate conversion, see “Corporate Conversion.” References in this prospectus to our capitalization and other matters pertaining to our equity prior to the corporate conversion relate to the capitalization and equity of Electrocore, LLC, and after the corporate conversion, to electroCore, Inc.
The consolidated financial statements included elsewhere in this prospectus are those of Electrocore, LLC and its subsidiaries and affiliate. We expect that our conversion from a Delaware limited liability company to a Delaware corporation will not have a material effect on our consolidated financial statements at the time of the corporate conversion.
Components of Our Results of Operations
Net Sales
We expect to generate the majority of our net sales from the United States. To date, we have generated revenue from the European CE Mark approval for gammaCore that we obtained in 2011 for five different indications, including primary headache. This allowed us to commercialize gammaCore in the European Economic Area and other countries that recognize the European CE Mark. Since 2013, we have generated revenue in Germany, United Kingdom, Australia, and Canada. We intend to explore select international markets to commercialize our gammaCore therapy as our resources permit, using direct, dealer and distributor sales models as the targeted market best dictates.
In April 2017, we received FDA clearance for gammaCore for the acute treatment of pain associated with episodic cluster headache. In July 2017, we began a product registry in the United States and as a result generated our first U.S. revenue relative to this FDA clearance.
We expect net sales of gammaCore to increase in the future as a result of new FDA clearances for indications for our therapy and as we expand our sales, marketing and distribution capabilities to support growth in the United States and in select markets internationally.
Cost of Goods Sold
Cost of goods sold consists primarily of direct material, direct labor and overhead costs. A significant portion of our cost of goods sold consists of overhead costs such as quality assurance, warehousing and shipment, facilities, depreciation on equipment and operations supervision and management. Due to our relatively low production volumes compared to our available assembling capacity, a large portion of our costs for our gammaCore therapy consists of overhead expense. If our production volumes increase as expected in the future, we anticipate that our per unit production costs will decrease.
Gross Profit
We calculate gross profit as net sales less cost of goods sold. Our gross profit has been and will continue to be affected by a variety of factors, including production volumes, assembly costs, product reliability and the implementation of cost-reduction strategies over time. We expect our gross profit to increase over time as our production volume increases and as we spread the fixed portion of our assembly and production overhead costs over a larger number of units produced, thereby significantly reducing our per unit assembly costs. However, our gross profit as a percentage of net sales, or gross margin, will be impacted by numerous factors including commencement of sales of gammaCore Sapphire in the United States, or any other future products, which may have higher product costs.
Research and Development
Our research and development expenses consist primarily of employee compensation, engineering, product development, tooling, proprietary data warehouse development and enhancements, quality
76
Table of Contents
assurance, clinical trial and regulatory expenses incurred in the development and FDA clearance of our gammaCore therapy. Research and development expenses also include consulting services, outside services and materials. We expense research and development costs as they are incurred.
Selling, General and Administrative
Our selling, general and administrative expenses consist primarily of personnel related costs (including compensation, benefits, and unit based compensation) for executive, finance, administrative and field based personnel, costs for commercial related infrastructure, and market development. In anticipation of clearance from the FDA and commencement of commercial sales in the United States, we incurred a significant increase in compensation costs as additional personnel were hired to oversee the execution of the commercial plan in the United States and Europe. Other significant expenses include costs associated with marketing and advertising, salesforce, professional fees for legal services, including legal services associated with our efforts to obtain and maintain broad protection for the intellectual property related to our products, rent, compliance, payor reimbursement development, accounting services, and consulting fees.
We expect selling, general and administrative expenses to continue to grow as we seek to execute our commercial and research and development plans. We also expect other non-employee-related costs, including outside services and accounting and legal costs to increase. The timing of these increased expenditures and their magnitude are primarily dependent on the commercial success and sales growth of gammaCore. In addition, we expect to incur increased selling, general and administrative expenses in connection with being a public company, which may further increase when we are no longer able to rely on certain “emerging growth company” exemptions we are afforded under the JOBS Act.
Amortization of Debt Discount and Issuance Costs
Amortization of debt discount and issuance costs consist primarily of the amortization of the fair value of the warrants, derivative options and common units issued in conjunction with our convertible bridge note financing, or Bridge Notes. These items were deemed a discount to the Bridge Notes and amortized on a straight line basis over the term of the Bridge Notes. In addition, the related issuance costs are similarly amortized over the term of the Bridge Notes.
Interest Expense
Interest expense consists of interest on our term loans and Bridge Notes which required the payment of interest based on a fixed interest rate over the length of the respective term loans and Bridge Notes.
Net Loss Attributable to Non-Controlling Interest
From our inception through December 31, 2017, we consolidated the financial results of our affiliate, electroCore (Aust) Pty Limited. Although we did not have a controlling ownership interest in electroCore (Aust) Pty Limited during that period, we determined that electroCore (Aust) Pty Limited was a variable interest entity, of which we were the primary beneficiary.
77
Table of Contents
Results of Operations
Year ended December 31, 2016 compared to Year ended December 31, 2017
The following table sets forth amounts from our consolidated statements of operations for the years ended December 31, 2016 and 2017.
| Year ended December 31, | ||||||||
| (in thousands) |
||||||||
| 2016 | 2017 | |||||||
| Net Sales |
$ | 254.1 | $ | |||||
| Costs of Goods Sold |
123.7 | |||||||
|
|
|
|
|
|||||
| Gross Profit |
130.4 | |||||||
| Research and Development |
7,971.3 | |||||||
| Selling, General and Administrative |
7,169.3 | |||||||
|
|
|
|
|
|||||
| Loss from Operations |
(15,010.2 | ) | ||||||
| Amortization of Debt Discount and Issuance Costs |
536.9 | |||||||
| Interest Expense |
234.4 | |||||||
| Net Loss Attributable to Non-controlling Interest | (44.1 | ) | ||||||
|
|
|
|
|
|||||
| Net Loss Attributable to Electrocore, LLC, subsidiaries and affiliate |
$ | (15,737.4 | ) | $ | ||||
|
|
|
|
|
|||||
Net Sales
Net sales increased $ to $ for the year ended December 31, 2017, from $0.3 million for the year ended December 31, 2016. This increase was primarily due to increased sales resulting from the establishment of our gammaCore product registry in the United States, as well as increased sales in Europe.
Costs of Goods Sold
Cost of goods sold increased $ to $ for the year ended December 31, 2017, from $0.1 million for the year ended December 31, 2016. This increase was due to an increase in the number of gammaCore units sold, and increased direct labor and overhead costs per unit as a result of additional staff required to assemble more units.
Gross Profit
Gross profit increased $ to $ for the year ended December 31, 2017 from $0.1 million for the year ended December 31, 2016. This increase was due to an increase in the number of gammaCore units sold, offset slightly by a $ increase in the cost per unit.
Research and Development
Research and development expenses increased $ to for the year ended December 31, 2017 from $8.0 million for the year ended December 31, 2016. The increase was the result of increased proprietary data warehouse development costs and associated software for gammaCore data collection of $ , offset by decreases in costs of clinical trials of $ , product research of $ , and quality assurance of $ .
Selling, General and Administrative
Selling, general and administrative expense increased by $ to $ for the year ended December 31, 2017 from $7.2 million for the year ended December 31, 2016. This increase is a result of increased personnel costs of $ related to newly hired personnel, increased legal costs of $ , and increased costs of $ related to consultants and service providers associated with the anticipated commercial launch of gammaCore and gammaCore Sapphire.
78
Table of Contents
Amortization of Debt Discount and Issuance Costs
Amortization of debt discount and issuance costs, which relate to our 2016-2017 Bridge Notes financing increased by $ to $ for the year ended December 31, 2017 from $0.5 million for the year ended December 31, 2016. These debt discounts and issuance costs were amortized on a straight-line basis over the term of the Bridge Notes that we issued in fiscal years 2016 and 2017. This increase was driven by the additional Bridge Notes that were issued in 2017 and the full amortization of the remaining debt discount and issuance costs as a result of the conversion of the debt to Series B Preferred Units in August 2017.
Interest Expense
Interest expense increased by $ to $ for the year ended December 31, 2017 from $0.2 million for the year ended December 31, 2016. This increase is primarily due to the issuance of additional Bridge Notes in 2017 of $ . The Bridge Notes and any related accrued interest were converted to Series B Preferred Units in August 2017.
Net Loss Attributable to Non-Controlling Interest
Net loss attributable to non-controlling interest increased by $ to $ for the year ended December 31, 2017 from $44.1 thousand for the year ended December 31, 2016. The increase is primarily due to losses related to our joint venture entity in Australia.
Net Loss Attributable to Electrocore, LLC, subsidiaries and affiliate
Net loss attributable to Electrocore, LLC, subsidiaries and affiliate increased by $ to $ for the year ended December 31, 2017 from $15.7 million for the year ended December 31, 2016. The increase is primarily due to the items described above.
Liquidity and Capital Resources
As of December 31 2017, we had an accumulated deficit of $ million. We anticipate that we will continue to incur losses for at least the next several years. We expect that our research and development expenses and selling, general and administrative expenses will continue to be significant and, as a result, we may need additional capital to fund our operations, which we may seek to obtain through a combination of equity offerings, debt financings, marketing and distribution arrangements and other collaborations, strategic alliances and licensing arrangements.
We have financed our operations to date primarily through the sale of our equity securities, including the issuance of equity securities upon the conversion of our convertible promissory notes, term loan and exercise of warrants. Our historical cash outflows have primarily been associated with cash used for operating activities such as the expansion and support of our sales and marketing infrastructure, an increase in our research and development activities, and other working capital needs. As of December 31, 2017, we had cash and cash equivalents of $ million. Cash in excess of immediate requirements is invested with a view to liquidity and capital preservation. Currently, our cash and cash equivalents are held in cash and money market bank accounts, all of which have original maturities of less than 90 days.
Until we can generate a sufficient amount of cash from operations, we expect to finance future cash needs through public or private equity or debt offerings. Additional capital may not be available on reasonable terms, if at all. If we are unable to raise additional capital in sufficient amounts or on terms acceptable to us, we may have to significantly scale back our operations or delay, scale back or discontinue the continuing development of gammaCore. If we raise additional funds through the issuance of additional debt or equity securities, it could result in dilution to our existing unitholders and increased fixed payment obligations, and these securities may have rights senior to those of our common
79
Table of Contents
units. If we incur indebtedness, we could become subject to covenants that would restrict our operations, such as limitations on our ability to incur additional debt, limitations on our ability to acquire, sell or license intellectual property rights and other operating restrictions that could adversely impact our ability to conduct our business. Any of these events could significantly harm our business, financial condition and prospects.
Cash Flows
The following table sets forth the significant sources and uses of cash for the periods noted below:
| Year ended December 31, | ||||||||
| 2016 | 2017 | |||||||
| (in thousands) |
||||||||
| Net cash provided by (used in) |
||||||||
| Operating activities |
$ | (13,225.8 | ) | |||||
| Investing activities |
— | |||||||
| Financing activities |
9,273.3 | |||||||
Operating Activities
Net cash used in operating activities was $ million for the year ended December 31, 2017, compared to $13.2 million for the year ended December 31, 2016. This increase in net cash used in operating activities of $ million was associated with changes in working capital of $ and an increase in net loss of $ . The changes in working capital reflect the increased inventory associated with our product registry and the anticipated launch of gammaCore as well as net changes associated with the timing of payments. Offsetting these uses was the amortization of debt discount and issuance costs of $ related to the Bridge Notes.
Investing Activities
Net cash used in investing activities was $ million for the year ended December 31, 2017 compared to $0 for the year ended December 31, 2016, and reflects the utilization of cash proceeds from issuance of the Bridge Notes and the sale of the Series B Preferred Units for the purchase of short-term investments.
Financing Activities
Net cash provided by financing activities was $ million for the year ended December 31, 2017 and $9.3 million for the year ended December 31, 2016, an increase of $ million. This increase was the result of the receipt of $ in net cash proceeds from the issuance of the Bridge Notes as well as $ in net cash proceeds from the issuance of the Series B Preferred Units.
Capital Resources
As of December 31, 2017, we had cash and cash equivalents of $ million and short-term investments of $ million. We believe that the anticipated net proceeds of this offering, together with our existing cash and cash equivalents, and short-term investments, will enable us to fund our operating expenses and capital expenditure requirements through at least the next 12 months. We have based these estimates on assumptions that may prove to be inaccurate or wrong, and we could exhaust our available capital resources earlier than we expect.
Series A Preferred Equity
From March 28, 2013 through September 2016, we received net proceeds of $50.7 million from the sale of Series A Preferred Units at an initial closing and several required milestone closings, several optional milestone closings, as well as from the conversion of certain loan amounts and the exercise of
80
Table of Contents
certain related warrants, net of related issuance costs. Investors in the Series A Preferred Unit financings directly or indirectly included the following related parties: Core Ventures II, LLC, or CV II, an entity that holds more than 5% of our outstanding units and in which Joseph P. Errico and Dr. Thomas J. Errico, two of our directors, have a pecuniary interest and for which they serve as managers with voting control; Peter S. Staats, M.D., our Chief Medical Officer and a former director, and Nicholas Colucci, a director, and Kathryn Theofilos, a former director of our company, invested through CV II; Merck Global Health Innovation Fund, LLC, or GHI, an entity for which one of our directors, David M. Rubin, serves as a Managing Director, and which owns greater than 5% of our outstanding units; and James L.L. Tullis, and the Tullis Opportunity Fund II, or TOP II, an entity in which Mr. Tullis, one of our directors, has a pecuniary interest and for which he serves as the managing partner of its general partner.
In September 2016, ECNG, LLC, or ECNG, a limited liability company in which Joseph P. Errico and Dr. Thomas J. Errico have a pecuniary interest and over which they have voting control, elected to convert $1.5 million in principal amount of Bridge Notes plus accrued interest of $26.4 thousand into 1,795,407 Series A Preferred Units. Kathryn Theofilos, a former director, also is a member of ECNG.
Term Loans
On December 22, 2015, Pacific Western Bank loaned us $1.25 million pursuant to a Loan and Security Agreement, which also provided for three additional term loans aggregating $6.25 million, available at various dates through June 2017. In connection with this loan, we issued 66,177 warrants to Pacific Western Bank to purchase our Series A Preferred Units at an exercise price of $0.85 per Unit. The warrants expire on December 22, 2025. In May 2016, the Company repaid the $1.25 million term loan balance in full and the Loan and Security Agreement was terminated.
On December 22, 2015, CV II also loaned us $1.25 million pursuant to a Loan and Security Agreement. In connection with this loan, we issued 66,177 warrants to CV II expiring on December 22, 2025 to purchase our Series A Preferred Units at an exercise price of $0.85 per unit. Pursuant to the terms of this loan, CV II elected to convert the loan of $1.25 million and related accrued interest of $49.9 thousand into approximately 1.5 million Series A Preferred Units in two installments in March 2016 and September 2016 at a price per unit of $0.85.
Bridge Notes
From September 2016 through June 2017, we issued an aggregate of $25.6 million of Bridge Notes to existing and new investors. The Bridge Notes accrued interest at an annual interest rate of 10% and had a maturity date one year from the date of issuance. Each Bridge Note was convertible into the equity securities issued in a subsequent equity financing that raised not less than $8.0 million, or a Qualified Equity Financing, at a 10% discount to the price of the equity securities issuable in the Qualified Equity Financing. The Bridge Notes were also convertible, at the option of the investors into Series A Preferred Units at $0.85 per Unit. Depending on the purchaser and amount invested, a purchaser of a Bridge Note also received either one half of one Common Unit, one Common Unit, or two Common Units for each dollar of principal amount of Bridge Note purchased.
Each purchaser of Bridge Notes after September 2016 also received warrant coverage of 20% of the principal amount of the Bridge Note. The Bridge Note warrants are exercisable from the date of the issuance of the Qualified Equity Financing until June 29, 2021 and entitle each holder to purchase an amount of securities issued in the Qualified Equity Financing equal to 20% of principal amount of the Bridge Notes purchased by each such investor divided by the price of the Qualified Equity Financing. The exercise price is equal to the Qualified Equity Financing price.
From December 2016 to June 2017, as compensation for placing Bridge Notes with investors in the principal amount of $8.1 million, our placement agents received cash of $0.8 million, 5.4 million
81
Table of Contents
common units, and 1.3 million warrants to purchase Series B Preferred Units at an exercise price of $0.70 per unit. Investors in the Bridge Notes financing included related parties as described in “Certain Relationships and Related Party Transactions.”
Series B Preferred Equity
In 2017, we issued and sold at a price of $0.70 per unit, in serial closings, $73.6 million of our Series B Preferred Units, inclusive of the automatic conversion of $25.6 million of our Bridge Notes plus $1.1 million of accrued and unpaid interest thereon. In connection with such closings, we also issued warrants for the purchase of 35.5 million common units at an exercise price of $1.25 per common unit. Investors in the Series B Preferred Unit financings included related parties as described in “Certain Relationships and Related Party Transactions.”
Contractual Obligations
In the normal course of business, we enter into obligations and commitments that require future contractual payments. The commitments result primarily from lease for office space and leased equipment. The following table summarizes our contractual obligations and commercial commitments as of December 31, 2017:
| Less than 1 year | 1 to 3 years | 3 to 5 years | More than 5 years | |||||||||||||
| Lease Rental Payments |
$ | 552,524 | $ | 1,687,764 | $ | 195,437 | — | |||||||||
The table above reflects only payment obligations that are fixed and determinable based on our current agreements. Our operating lease commitment relates to the facility leased for our corporate headquarters in Basking Ridge, New Jersey.
Off-Balance Sheet Arrangements
We did not have during the periods presented, and we do not have any off-balance sheet arrangements, as defined in the rules and regulations of the SEC.
Quantitative and Qualitative Disclosures About Market Risk
We develop our products in the United States and sell those products into more than four countries. As a result, our financial results could be affected by factors such as changes in foreign currency exchange rates or weak economic conditions in foreign markets. Most of our sales in Europe are denominated in the U.S. Dollar and Euro. As our sales in currencies other than the U.S. dollar increase, our exposure to foreign currency fluctuations may increase. In addition, changes in exchange rates also may affect the end-user prices of our products compared to those of our foreign competitors, who may be selling their products based on local currency pricing. These factors may make our products less competitive in some countries.
If the U.S. dollar uniformly increased or decreased in strength by 10% relative to the currencies in which our sales were denominated, our net income would have correspondingly increased or decreased by an immaterial amount for the year ended December 31, 2017.
Our exposure to market interest rate risk is confined to our cash and cash equivalents and short-term investments. As of December 31, 2017, we had $ million in cash and cash equivalents and $ in short-term investments. The goals of our investment policy are preservation of capital, fulfillment of liquidity needs and fiduciary control of cash and investments. We also seek to maximize income from our investments without assuming significant risk. To achieve our goals, we may maintain a portfolio of cash equivalents and investments in a variety of securities of high credit quality. The securities in our investment portfolio, if any, are not leveraged, are classified as either available for sale or
82
Table of Contents
held-to-maturity and are, due to their very short-term nature, subject to minimal interest rate risk. We currently do not hedge interest rate exposure. Because of the short-term maturities of our cash equivalents, we do not believe that an increase in market rates would have any material negative impact on interest income recognized in our statement of operations. We have no investments denominated in foreign currencies and therefore our investments are not subject to foreign currency exchange risk.
All of the potential changes noted above are based on sensitivity analyses performed on our financial position as of December 31, 2017.
Critical Accounting Policies and Estimates
The preparation of our financial statements are in accordance with accounting principles generally accepted in the United States. We are required to make estimates and assumptions that affect the reported amounts of assets and liabilities as of the date of the consolidated financial statements, the reported amounts of net sales and expenses during the reporting periods and the related disclosures in the consolidated financial statements. We believe that the following accounting policies described in Note 2: “Summary of Significant Accounting Policies” in the audited consolidated financial statements included elsewhere in this prospectus, are critical because they involve a higher degree of judgment and uncertainty. As a result, these accounting policies could materially affect our financial statements.
On an ongoing basis, we evaluate these estimates and judgments based on historical experiences and various other factors that are believed to reflect the current circumstances. While we believe our estimates, assumptions and judgments are reasonable, they are based on information presently available. Actual results may differ significantly from these estimates due to changes in judgments, assumptions and conditions as a result of unforeseen events or otherwise, which could have a material impact on our financial position and results of operations.
Revenue Recognition
We operate in one reportable segment and all of our net sales are derived from sales of our gammaCore product, net of specialty pharmaceutical distribution discounts. Products are sold to a specialty pharmaceutical distributor. Revenue is recognized when persuasive evidence of an arrangement exists, our customer takes ownership and assumes risk of loss, the selling price is fixed or determinable and collection is reasonably assured. We expect to receive payment on all of our customer receivables within one year and therefore classify all receivables as current assets.
At the current time, we do not provide an allowance for returns. Therapy delivered from our gammaCore products and subsequent refills are sold in 31-day increments to the specialty pharmaceutical distributor. Our products stop delivering therapy after 31 days, at which time the patient discards the product, in the case of gammaCore, and receives a new 31-day gammaCore product. In the case of the gammaCore Sapphire, patients require a prescription refill to receive the next 31 days of therapy via our refill RFID card.
We expense the cost, as incurred, of product damaged as a result of shipping to our specialty pharmaceutical distributors. This expense, historically, has been immaterial.
Accounts receivable are net of an allowance for doubtful accounts, which are accounts from which payment is not expected to be received although product was provided and revenue was earned. Receivables are written off when deemed uncollectible. Recoveries of receivables previously written off are recorded when received. To date, we have not provided an allowance for doubtful accounts, based on historical experience.
83
Table of Contents
Inventories
We value inventory at the lower of cost or market (net realizable value). Cost is determined by the weighted average cost method. This policy requires us to make estimates regarding the market value of our inventory, including an assessment of excess or obsolete inventory. We evaluate inventory for excess quantities and obsolescence based on an estimate of the future demand for our product within a specified timeframe, and record an allowance to reduce the carrying value of inventory as determined necessary. The estimates we use for demand are also used for near-term capacity planning and inventory purchasing and are consistent with our revenue forecasts. If our actual demand is less than our forecast demand, we may be required to take additional excess inventory charges, which would decrease gross margin and adversely impact net operating results in the future.
Income Taxes
Currently, we are a limited liability company and therefore tax attributes are passed through to our members. Prior to the closing of this offering, we will convert to a Delaware corporation. We will be taxed at the rates applicable within each jurisdiction in which we will operate and/or generate revenue. The composite income tax rate, tax provisions, deferred tax assets and deferred tax liabilities will vary according to the jurisdiction in which profits arise. Tax laws are complex and subject to different interpretations by management and the respective governmental taxing authorities, and require us to exercise judgment in determining our income tax provision, our deferred tax assets and liabilities and the valuation allowance recorded against our net deferred tax assets.
Research and Development Expenses
We incur significant expenditures on research and development costs, including clinical testing for regulatory purposes and these expenses have been expensed as incurred. Our research and development expenses primarily consist of pilot and pivotal clinical trials relative to current and future therapeutic indications, product engineering, technical updates, quality assurance and regulatory expenses. Additionally, these expenses are comprised of development and enhancements to our proprietary data warehouse, which maintains patient product serial numbers and interacts in real time, with a device placed at the specialty pharmacy to program RFID refill cards. Research and development expenses also include employee unit-based compensation, consulting services, outside services, materials, and supplies relating to clinical trials including products revisions, data statistics and patient recruitment.
Unit-Based Compensation
We record compensation costs related to our unit-based awards, which currently include profits interests units, based on the fair value of such awards. Compensation expense is recognized over the vesting period during which an employee is required to provide services in exchange for the award. All unit-based awards are expensed on a straight-line basis over the vesting period, which is generally four years.
Measurement of unit-based payment transactions with non-employees is based on the fair value of whichever is more reliably measurable: (a) the goods or services received; or (b) the equity instruments issued. The fair value of the unit-based payment transaction is determined at the earlier of performance commitment date or performance completion date.
The estimation of the fair value of each profits unit grant or issuance on the date of grant involves numerous assumptions by management. Although we calculate the fair value under the Black-Scholes option pricing model, which is a standard option pricing model, this model still requires the use of numerous assumptions, including, among others, the expected life (turnover), volatility of the underlying equity security, a risk free interest rate and expected dividends. We do not have publicly traded equity and have a limited operating history and a lack of company-specific historical and implied volatility data, and therefore we have estimated stock price volatility based upon an index of the historical volatilities of
84
Table of Contents
a group of publicly-traded industry peer companies. We have estimated the expected term of our profits interest units using the “simplified” method, whereby the expected life equals the average of the vesting term and the original contractual term of the option. The use of different values by management in connection with these assumptions in the Black-Scholes option pricing model could produce substantially different results.
Determination of the Fair Value of Common Units
As there has been no public market for our common units to date, the estimated fair value of our common units has been supported by third-party valuations with input of objective and subjective factors that management believe are relevant. Our third-party valuations resulted in valuations of our common units of $0.14 per unit as of December 31, 2016, $ per unit as of June 30, 2017, $ per unit as of September 30, 2017, and $ per unit as of December 31, 2017. These third-party valuations were performed in accordance with the guidance outlined in the American Institute of Certified Public Accountants’ Accounting and Valuation Guide, Valuation of Privately-Held-Company Equity Securities Issued as Compensation.
Our third-party valuation of common units was prepared using the discounted cash flow, or DCF, method, a form of the income approach, to estimate our equity value. In order to estimate equity value, the DCF method uses the estimated present value of future net cash flows for the expected life of the related assets or business, discounted at a rate of return that considers the relative risk of achieving those cash flows, the time value of money and the current stage of development of the business. The total fair value of equity on a marketable basis was then allocated between each class of equity, including common units, preferred units, profits interests, and warrants, applying a hybrid method of allocation. Under the hybrid method, a probability-weighted expected return method and an option pricing model were utilized.
The assumptions underlying these valuations represent management’s best estimates, which involve inherent uncertainties and the application of management judgment. As a result, if factors or expected outcomes change and we use significantly different assumptions or estimates, our share-based compensation expense could be materially different.
Following the closing of this offering, the fair value of our common shares will be determined based on the quoted market price of our common shares.
Profits Interests Granted
The following table summarizes by grant period the number of Profits Interests units granted by us during 2017 as well as the estimated fair value of such grants as of the grant date:
| Three months ended |
Number of units | Fair value per underlying unit at date of grant | ||||||||
| March 31, 2017 |
45,000 | $ | ||||||||
| June 30, 2017 |
1,810,000 | $ | ||||||||
| September 30, 2017 |
11,170,335 | $ | ||||||||
| December 31, 2017 |
7,193,754 | $ | ||||||||
Bridge Notes and Warrants
The Bridge Notes, common units and warrants to purchase securities in the Qualified Equity Financing (and, for issuances before October 2016, warrants to purchase Series A Preferred Units) were issued to investors simultaneously in exchange for cash equal to the principal amount of the Bridge Notes. In addition, the Bridge Notes were issued with an embedded automatic conversion feature in which
85
Table of Contents
outstanding Bridge Notes are converted to Series B Preferred Units upon occurrence of the Qualified Equity Financing. Each of these separate financial instruments and embedded features require separate accounting.
The proceeds of the bridge financing transactions were required to be allocated to each of the Bridge Notes, Common Units, and warrants. In addition, the embedded option to convert to Series A Preferred Units and the automatic conversion feature to Series B Preferred Units were determined to be embedded derivatives that require bifurcation from the Bridge Notes and separate accounting.
The warrants were evaluated by management and determined to be liability classified. As such, the warrants are measured at fair value with changes in fair value recognized in net income. After subtracting the fair value of the warrants at issuance, the remaining proceeds were allocated to the Bridge Notes (inclusive of the embedded automatic conversion feature) and common units at their relative fair values. The embedded option to convert Series A Preferred Units and the automatic conversion feature to Series B Preferred Units was then separated from the Bridge Notes and measured at fair value with changes in fair value recognized in net income. The residual amount of proceeds were then allocated to the Bridge Notes.
As a consequence of the allocation of proceeds of the bridge financing to the financial instruments and embedded derivative described above, the Bridge Notes were issued at a discount. This discount has been amortized over the life of the Bridge Notes.
Valuation of Bridge Notes
In order to allocate proceeds of the bridge financing transactions, a determination of the fair value of the common unit, warrant and conversion features of the Bridge Notes was required. We used an alternative discounted cash flow method to value the Bridge Notes. More specifically, we determined the fair value of the straight convertible debt component by discounting principal and interest payments back to the present value at a 40% required rate of return over a dollar-weighted average term of 0.69 years as of December 31, 2016 and as of June 30, 2017 we used a 45% required rate of return over a dollar-weighted average term of 0.17 years. As of December 31, 2016 and June 30, 2017, we determined the fair value of the embedded value of the option’s ability to convert at a 10% discount into the next Qualified Equity Financing. For June 30, 2017, this was done by discounting the difference between the aggregate Bridge Note principal plus interest at a 10% discount to the next Qualified Equity Financing and the aggregate Bridge Note principal plus interest at a 45% required rate of return less a 10% discount for lack of marketability times a 95% probability of a Qualified Equity Financing closing prior to the maturity date of the Bridge Note. For December 31, 2016, this was done by discounting the difference between the aggregate Bridge Note principal plus interest at a 10% discount to the next Qualified Equity Financing and the aggregate Bridge Note principal plus interest at a 50% required rate of return less a 10% discount for lack of marketability times an 80% probability of a Qualified Equity Financing closing prior to the maturity date of the Bridge Note. Changes to the assumptions used in such valuation could have a significant impact on these fair values.
Valuation of Embedded Derivative Liability Associated with Bridge Notes
The embedded derivative liability relating to the debt component of the Bridge Notes is measured at fair value and is subsequently remeasured at fair value at each reporting date. Changes in the fair value of the derivative liability are recognized as a component of amortization of debt discount and issuance cost in our consolidated statement of operations. We continued to recognize changes in the fair value of the derivative liability embedded in the Bridge Notes until the conversion into the Qualified Equity Financing, which occurred in connection with the conversion of the Bridge Notes into Series B Preferred Units in August 2017.
86
Table of Contents
The embedded option to convert to Series A Preferred Units was deemed to be de minimus. The embedded derivative liability related to the automatic conversion of the Bridge Notes in the Qualified Equity Financing was recorded at fair value using an alternative discounted cash flow method. The derivative liability related to the Bridge Notes was recorded at fair value determined by using an alternative discounted cash flow method. This method of valuation involves using inputs such as a 50% required rate of return, an 80% probability of a Qualified Equity Financing closing prior to the maturity of the Bridge Notes, and an option’s ability to convert at a 10% discount into the expected next Qualified Equity Financing. Changes to the assumptions used in such valuation could have a significant impact on the fair value of the derivative liability.
Valuation of Warrant Liability
As discussed above, the warrants to purchase securities in the Qualified Equity Financing were determined to be liability classified. Management determined that such warrants potentially obligated the Company to repurchase or redeem the future Qualified Equity Financing, as the terms of the Qualified Equity Financing was unknown at the time the warrants were issued alongside the Bridge Notes.
The warrants are recorded as a liability on our balance sheet at their fair value and are revalued at each reporting date, with fair value changes recognized as amortization of debt discount and issuance cost in the consolidated statement of operations. We will continue to adjust the liability for changes in fair value until the earlier of the exercise or expiration of the warrants, or the issuance of securities in a Qualified Equity Financing, at which time the classification of the warrants as liabilities or as equity is reassessed. We estimate the fair value of the liability using option pricing models and assumptions that are based on the individual characteristics of the warrants or instruments on the valuation date, including assumptions for expected volatility, expected life, yield, and risk-free interest rate.
Valuation of Series B Preferred Units and Warrants
In August 2017 the Company simultaneously issued Series B Preferred Units (which constituted the Qualified Equity Financing noted above) and warrants to purchase Common Units for $1.25 per unit. The Series B Preferred Units and warrants were evaluated by management and determined to be equity classified. Both of these instruments require separate accounting and the proceeds of the issuance of the Series B Preferred Units were required to be allocated to each instrument on a relative fair value basis.
In order to allocate proceeds of the issuance of Series B Preferred Units and warrants to purchase Common Units, a valuation of both instruments at fair value was required. We used a hybrid method to value the Series B Preferred Units and warrants to purchase Common Units. Under the hybrid method, a probability-weighted expected return method and an option pricing model were utilized.
Recent Accounting Pronouncements
A description of recently issued accounting pronouncements that may potentially impact our financial position and results of operations is disclosed in Note 2 to our consolidated financial statements appearing at the end of this prospectus.
Emerging Growth Company Status
In April 2012, the JOBS Act was enacted by the federal government. Section 107 of the JOBS Act provides that an emerging growth company can take advantage of the extended transition period for complying with new or revised accounting standards. Thus, an emerging growth company can delay the adoption of certain accounting standards until those standards would otherwise apply to private companies. We have irrevocably elected to “opt out” of this provision and, as a result, we will comply
87
Table of Contents
with new or revised accounting standards when they are required to be adopted by public companies that are not emerging growth companies.
In addition, as an emerging growth company, we will not be required to provide an auditor’s attestation report on our internal control over financial reporting in future annual reports on Form 10-K as otherwise required by Section 404(b) of the Sarbanes-Oxley Act.
88
Table of Contents
Overview
We are a commercial-stage bioelectronic medicine company with a platform non-invasive vagus nerve stimulation therapy initially focused on neurology and rheumatology. Our therapy, gammaCore, has pharmacologic effects on the peripheral and central nervous systems, which modulate neurotransmitters and immune function. gammaCore is FDA-cleared for the acute treatment of pain associated with migraine and episodic cluster headache in adults. Based on our clinical data, we are pursuing label expansions for the prevention of migraine, migraine in adolescents and post-traumatic headache, and we are also engaging in clinical development for potential new labeling claims in rheumatology, including Sjôgren’s syndrome and rheumatoid arthritis.
gammaCore is the first FDA-cleared, prescription-only VNS therapy administered in discrete doses using a proprietary, simple-to-use handheld delivery system. Our therapy activates the therapeutically relevant fibers in the vagus nerve. This is enabled by our proprietary high-frequency burst waveform that safely and comfortably passes through the skin and stimulates the targeted nerve fibers. The modulation of neurotransmitters by our therapy has a similar pharmacological effect to that of multiple classes of medications, including selective serotonin reuptake inhibitors, serotonin norepinephrine reuptake inhibitors, GABA analogues, acetylcholine esterase inhibitors and triptan medications, all of which are commonly prescribed. Research indicates that VNS therapy also modulates the immune system to produce anti-inflammatory effects comparable to therapies that inhibit inflammatory cytokines.
Migraine is a debilitating primary headache condition characterized by severe throbbing pain or a pulsing sensation, usually on one side of the head. Migraine affects approximately 12% of the adult population globally and disproportionately impacts women of childbearing years. In the United States, there are approximately 36 million migraine sufferers and, according to the U.S. Pharmacist, a leading pharmacy publication, upwards of 60% of the migraine patient population is dissatisfied with, or has contraindications to, the current standard of care treatments for migraine, such as triptan medications. We estimate the total addressable market for the acute treatment of migraine in the United States in 2018 will be approximately $3.8 billion. Five million migraine sufferers are treated by approximately 1,100 U.S. headache specialists, primarily neurologists.
Cluster headache, or CH, is a series of relatively short but extremely painful headaches that has been described by patients and physicians as one of the most painful conditions in medicine. The suicide rate among these patients is 20 times the U.S. national average, leading to the condition being referred to as the “suicide headache.” There are approximately 350,000 CH sufferers in the United States, approximately 225,000 of whom seek treatment each year primarily from the same headache specialists who treat migraine, and we estimate the total addressable U.S. market for the acute treatment of these patients in 2018 is approximately $400 million. We believe the significant unmet need and highly-targeted market of CH represents an ideal entry point for our therapy into the headache market, providing an opportunity to gain relevance with treating clinicians in order to support an expansion into migraine. Prior to gammaCore, there was only one FDA-approved, commercially available acute CH treatment, injectable sumatriptan, and according to a 2016 market research survey, 87% of respondents reported dissatisfaction with the then-available treatment options for CH.
Historically, vagus nerve stimulation, or VNS, required a highly invasive surgical procedure to implant a costly medical device that cannot be removed. Due to these limitations, VNS has only been indicated for the most severe patients. gammaCore stimulates the vagus nerve through an easy-to-use handheld delivery system dispensing therapy on a 31-day prescription basis, enabling access to VNS therapy to a much broader patient population than previously possible. gammaCore’s successor, gammaCore Sapphire, is a rechargeable and reloadable version of our product intended for multi-year use. It is
89
Table of Contents
activated on a monthly basis through the input of a unique, prescription-only authorization code, delivered via a radio-frequency identification, or RFID, card. In the future, this authorization code may be delivered through the internet, leveraging the Bluetooth capabilities of the gammaCore Sapphire.
Following the FDA’s review and grant of our de novo application, in April 2017, our gammaCore therapy was FDA-cleared for commercial sale in the United States for the acute treatment of pain associated with episodic cluster headache, or eCH, in adults. A de novo review is a regulatory pathway for products deemed by the FDA to be low to moderate risk, but without an applicable predicate. With the successful completion of our de novo review, a new regulatory category was created, which enabled us to seek label expansion for our product through the less burdensome 510(k) pathway, utilizing our own product as the predicate. The new regulatory category for external vagal nerve stimulation resulting from our de novo review encompasses the treatment of all headache conditions. gammaCore Sapphire was cleared by the FDA through the 510(k) pathway in December 2017. In January 2018, the FDA cleared our gammaCore therapy as an acute treatment for pain associated with migraine in adults.
In addition to our lead indications for the acute treatment of pain associated with both migraine and eCH in adults, we are also pursuing clinical programs to support label expansion filings for adolescent migraine, headache prevention indications, and the treatment of post-traumatic headache. Table 1 below summarizes our headache-related areas of focus for gammaCore:
Table 1: Our Headache Pipeline
| 1. | The gammaCore product registry for the acute treatment of cluster headache constitutes our initial commercialization efforts for our product. The full product launch is expected in the second quarter of 2018. |
Modulation of the peripheral immune system by VNS provides mechanistic support for the study of gammaCore in the treatment of inflammatory disorders. Based on initial positive results from our pilot trials, we expect to initiate a series of pivotal trials designed to support regulatory approvals in multiple rheumatologic conditions, including Sjôgren’s syndrome and rheumatoid arthritis.
Background of VNS
The vagus nerve is the largest and most extensive cranial nerve, connecting the brainstem to nearly every organ in the chest and abdomen, including the heart, lungs, liver, stomach, spleen, kidneys, and digestive tract, as shown in Figure 1 below.
90
Table of Contents
Figure 1: The distribution of the vagus nerve to multiple organs

Activation of the vagus nerve causes the release of neurotransmitters, both in the central and peripheral nervous systems, modulating how the brain and peripheral organs function. In the central nervous system, VNS activates areas of the brainstem that release norepinephrine, acetylcholine, serotonin, GABA and other important neurotransmitters. These effects can be used to treat multiple conditions, including epilepsy, depression and headache. The impact of neurotransmitter modulation in the periphery has been shown to have multiple beneficial effects, including the reduction of systemic inflammatory cytokines. VNS is being studied for use in a number of inflammatory conditions, including Sjôgren’s syndrome, rheumatoid arthritis and Crohn’s disease.
Over the past two decades, the body of scientific evidence in support of VNS in multiple medical conditions has been growing. However, this potential has remained unfulfilled because the therapy could only be delivered using electrodes wrapped around the vagus nerve, connected to a signal generator implanted in the chest wall. To implant these devices, the vagus nerve must be surgically exposed from its anatomical position, entwined with the carotid artery.
Prior to gammaCore, VNS was only accessible to the most refractory patients, who were willing to endure surgery, and payors were forced to spend tens of thousands of dollars prior to determining the efficacy of the post-surgical therapy for those patients. With the clearance of gammaCore, this safe and effective therapy can now be noninvasively self-administered, at a fraction of the initial cost, exponentially expanding its accessibility for the potential treatment of multiple medical conditions.
Preclinical Evidence of gammaCore’s Activation of the Vagus Nerve
During the development of gammaCore, we pioneered a series of inventions that enable the comfortable passage of our proprietary therapeutic signal to specifically targeted fibers of the vagus nerve. Confirmation that our delivery technology successfully activates the vagus nerve has been published by independent researchers who performed electromagnetic field modeling demonstrating that our therapy establishes the necessary charge gradients in the targeted nerve fibers, without depositing a net charge to the overall tissue that would cause significant discomfort.
Confirmation of this electromagnetic field modeling has been conducted in humans, and published by multiple independent research groups. Specifically, these experiments show that gammaCore produces
91
Table of Contents
changes in electroencephalography, or EEG, similar to what has been observed with VNS delivered using surgically implanted devices, and does so in a dose-dependent manner, consistent with chemical and biologic pharmaceutical products.
In addition, we have sponsored research by multiple groups of independent scientists to demonstrate that gammaCore activates the critical areas in the brainstem necessary to provide clinically beneficial effects. These studies included both functional magnetic resonance imaging, and magnetoencephalography, both of which showed that gammaCore activates critical areas in the brainstem, including the substantia nigra, the nucleus raphe magnus, or NRM, the periaqueductal gray, or PAG, and the thalamus.
Additional studies we sponsored showed that when these areas of the brainstem were activated, there was an upregulation in the neurotransmitters that modulate pain, including norepinephrine, GABA, acetylcholine, and serotonin.
VNS modulates not only the functional state of the central nervous system, but also the activation state of the immune system. We have sponsored multiple studies looking at the effects of gammaCore on the levels of inflammatory cytokines and other biomarkers of inflammation. These studies show that gammaCore is capable of suppressing TNF-a, IL-1ß, and IL-6, both in the central nervous system and in the periphery.
Our Therapy Delivery Platform
Our gammaCore therapy is the first and only treatment that non-invasively activates the therapeutically relevant fibers in the cervical trunk of the vagus nerve. More specifically, our therapy employs proprietary signals that are capable of passing through skin while minimizing the activation of skin pain receptors.
Our therapy is prescription-only, and like medications delivered by metered-dose inhalers, patients self-administer discrete doses using a handheld unit that can be either disposable or reusable. In either case, the therapy is dispensed through a monthly prescription from a specialty pharmacy.
gammaCore Sapphire is the non-disposable, rechargeable and reloadable option for patients requiring therapy on an on-going basis. It is refilled monthly through the input of a unique, prescription-only authorization code, delivered through an RFID card dispensed by mail through our specialty pharmacy partner. In the future this refill may be dispensed directly through the internet using Bluetooth.
Competitive Strengths
We believe the competitive strengths of our company and our novel and proprietary self-administered bioelectronic therapy include:
| • | Innovative bioelectronic medicine approach. Our gammaCore therapy uses a proprietary electric signal to safely deliver bioelectronic medicine, which causes targeted pharmacologic-like changes in neurotransmitter expression and in the immune system, without systemic exposure to exogenous chemicals. |
| • | Our non-invasive therapy unlocks the long-held potential of VNS. VNS therapy can, for the first time, be delivered safely and comfortably through the skin using gammaCore. This eliminates the need for costly, invasive surgery that requires the implantation of a permanent medical device. VNS therapy is no longer reserved for the most refractory patients, and is now a first-line treatment option. |
| • | Commercializing our therapy through traditional pharmaceutical channels. Our non-invasive delivery modality permits medical professionals to prescribe VNS through the same channel they would any other specialty medication. Refills delivered on a monthly basis enable us to seek widespread commercial payor coverage and reimbursement under a traditional pharmaceutical model. |
92
Table of Contents
| • | Highly scalable and low investment manufacturing with digital refills. Our low manufacturing and assembly costs allow us to scale to meet demand with minimal additional investment. Refills through RFID or Bluetooth may offer attractive gross margins. |
| • | Potential for rapid label expansion in headache and regulatory approval in additional indications. The safety profile of gammaCore enabled us to utilize the de novo regulatory pathway through which the FDA established a new therapeutic category: external vagal nerve stimulator for the treatment of headache. Through the 510(k) pathway, we received clearance for our gammaCore therapy for the acute treatment of pain associated with migraine in adults in January 2018. We believe a similar regulatory pathway may be available to us for additional indications in rheumatology. |
| • | Broad intellectual property protection. Among our key issued patents, we have coverage on using our high-frequency burst signal for treating disorders until 2031, the low-pass filtering of that signal to ensure comfortable transmission through the skin until 2031, the non-invasive treatment of headache conditions until 2029, and the remote network-enabled communication for the delivery of neuromodulation therapy for a broad range of medical conditions until 2033. |
| • | Highly experienced management team. Our management team includes a diverse group of executives with significant experience in senior positions in the pharmaceutical and medical device industries, including positions at Pfizer, Merck, Novartis, Stryker and Zimmer Biomet. Members of our team have been involved in the launch and marketing of products including Motrin, Celebrex, and the migraine drugs Axert and Maxalt. Our team’s pharmaceutical experience in clinical development, sales, marketing and reimbursement, and its medical device experience in research, development and regulatory affairs, allow us to pursue our strategy and growth plans. |
Our Strategy
Our goal is to be a leader in bioelectronic medicine by using our proprietary non-invasive VNS platform therapy to deliver better patient outcomes. The key elements of our strategy include:
| • | Drive acceptance of our gammaCore products as a leading headache therapy, introducing it in cluster headache and expanding into migraine. We plan to establish gammaCore as the first-line treatment option for neurologists when treating eCH patients, who have few alternative treatment options available to them. We will then leverage this position to expand into the broader headache market for migraine in the second quarter of 2018. |
| • | Drive reimbursement of our therapy. We are actively engaging with over 50 national and regional commercial insurance payors in the United States with the goal of securing reimbursement coverage as a pharmacy benefit. To date, we have secured pharmacy benefit reimbursement for 2.1 million commercial lives, and are in active clinical review discussions with more than a dozen additional insurance plans covering approximately 120 million additional commercial lives. |
| • | Build a leading commercial presence. We have established a robust specialty distribution channel with a patient-focused concierge service to quickly onboard patients and manage payor interactions. We are expanding our direct sales force to target high prescribing neurology specialists and headache centers that originate the substantial majority of new prescriptions for severe headache patients in the United States. In the first year following our commercial launch into migraine, we expect to be able to target 120 national headache centers and approximately 6,000 physicians. |
| • | Rapidly advance our pipeline. In 2018, we expect to initiate pivotal trials to support potential label expansion in headache, including additional trials in migraine prevention and |
93
Table of Contents
| migraine in adolescents. In 2018, we also expect to initiate our first major trials in rheumatology, including pivotal trials in Sjôgren’s syndrome and rheumatoid arthritis. Over the next 24 months, we anticipate additional sponsored pilot trials will be conducted in both neurology and rheumatology. |
Our Lead Indications in Headache
In January 2018, gammaCore was cleared by the FDA for commercial sale in the United States as an acute treatment for pain associated with migraine in adults. This followed the April 2017 grant of our de novo application by the FDA that cleared our gammaCore for commercial sale in the United States for the acute treatment of pain associated with episodic cluster headache, or eCH, in adults. In accordance with our strategy to establish gammaCore as the preferred treatment for neurologists across headache, we initially targeted a high unmet need population in eCH to establish relevance with prescribing clinicians and gain reimbursement from payors. From this position, we are now expanding into the broader headache market, starting with migraine.
CH sufferers experience a series of relatively short but extremely painful headaches that have been described by patients and physicians as one of the most painful conditions in medicine. CH predominantly affects males in their prime earning ages of 20 to 50, with bouts of frequent attacks, known as cluster periods, often occurring every other day, and up to eight times a day. Individual attacks can last from 15 minutes to as long as three hours, with these frequent attacks continuing for a prolonged period. Among CH patients, 85% to 90% experience eCH, with cluster periods, or bouts, lasting from two to 12 weeks, followed by a remission period often cycling into bout twice per year. Chronic CH, or cCH, patients experience no periods of remission or remission periods of less than 3 months in a 12-month period. The suicide rate of CH sufferers is 20 times the U.S. national average, leading to the condition being referred to as the “suicide headache.” In the United States, CH affects approximately 350,000 people. There is only one FDA-approved commercially available pharmaceutical option for acute CH treatment, and none for its prevention.
Migraine, the third most common disease in the world, is a debilitating primary headache condition characterized by severe throbbing pain or a pulsing sensation, usually on one side of the head, often associated with nausea and sensitivity to light and sound. Migraine impacts more than 36 million people in the United States, disproportionately affecting women of childbearing years, with peak onset during the adolescent ages of 12 to 16. While migraine sufferers have a number of approved and available treatments, the side effects and incomplete efficacy of these options continues to drive a high level of dissatisfaction with current therapies.
Our first FDA clearance, received following the grant of our de novo application, was for the acute treatment of eCH in adults, and is supported by two pivotal trials: our ACT 1 trial, or ACT 1, and our ACT 2 trial, or ACT 2. The primary endpoints of these trials were pain reduction and pain-freedom within 15 minutes of the onset of the attack, respectively. While neither trial reached statistical significance with respect to its primary endpoint in the combined eCH and cCH populations, both trials reached statistical significance (ACT 1; 34.2%; ACT 2; 47.5%; p<0.01 in each trial) on the primary endpoint in the eCH cohort.
Our FDA clearance for the acute treatment of migraine in adults is principally supported by our pivotal trial, PRESTO. The primary endpoint of PRESTO was pain-freedom at 120 minutes. While this trial did not reach statistical significance with respect to its primary endpoint, statistical significance was achieved for complete pain relief at 30 minutes (12.7%; p=0.01), and maintained at 60 minutes (21.0%; p=0.02), and under a repeated-measures analysis, through the full 120-minute period (30.4%; p=0.01).
94
Table of Contents
The Limitations of Pharmaceutical Treatment Options in Headache
There is only one FDA-approved commercially available pharmaceutical treatment for the acute treatment of CH, injectable sumatriptan. Patients have typically been limited to fewer than 10 injections per month, primarily due to cost and toxicity. In addition, the technical difficulty of subcutaneously self-injecting a medication during a CH attack may also limit use of this therapy. As a result, patients typically have enough medication to treat, on average, only a fraction of their monthly CH attacks. There are no approved treatments for the prevention of CH, driving patients to use off-label medications, such as lithium, valproic acid and high-dose verapamil, which have unproven efficacy and the potential for significant toxicity, including adverse cardiac events. In a 2016 market research survey of CH patients, 87% of the respondents were dissatisfied with the then-available treatment options.
Although there are more prescription therapies available for migraineurs than CH sufferers, according to the U.S. Pharmacist, a leading pharmacy publication, upwards of 60% of the migraine patient population has reported dissatisfaction with, or has contraindications to, the current standard of care treatments for migraine. These medications include triptans, ergotamines and anti-epileptic medications. Despite the fact that neurologists recognize the limited efficacy of, and the potential for abuse associated with, opioids, they continue to be prescribed at high rates, particularly in emergency departments for the treatment of migraine. Many other primary headache conditions, and secondary headaches, such as post-traumatic headache, have proven refractory to pharmaceutical interventions, presenting a significant unmet need in the market.
Cluster Headache
The Condition. CH sufferers experience a series of relatively short but extremely painful headaches. The clinical criteria for CH define the attacks as frequent, severe, short-duration head and eye socket pain, accompanied by autonomic symptoms, such as sweating, tearing, swelling of the eyelid, and sinus congestion on only one side of the face. CH patients are typically agitated, pacing, moaning and sobbing, and often beat or claw at their heads in desperation.
CH patients, and the physicians who treat them, describe the attacks as one of the most painful conditions in medicine. The prevalence of CH is three times higher in males than in females, and peaks in their prime earning ages of 20 to 50. Attacks can last from 15 minutes to as long as three hours, with these frequent attacks occurring, on average, twice per day. For some, they can occur as many as eight times per day. CH is known as the “suicide headache” because the suicide rate among CH sufferers is a reported 20 times higher than that for the general population in the United States. During attacks, CH patients have been known to harm themselves as a distraction from the excruciating pain.
CH can be either episodic, eCH, or chronic, cCH. eCH sufferers experience alternating periods of attacks and remission lasting weeks or months. cCH sufferers experience extended periods of attacks, occurring without a remission period, or with remissions lasting less than three months, for at least one year.
Prevalence and market size. The estimated prevalence of CH in the United States ranges from 0.1% to 0.2% of the total population, with consensus around 350,000 as the number of affected patients, of which 225,000 patients seek medical treatment annually. eCH patients average approximately four months per year in bout. We estimate the total addressable market for the acute treatment of eCH in the United States in 2018 will be approximately $400 million.
Economic Burden. According to a recent published study in The American Journal of Managed Care, the overall average medical costs for eCH patients over a three-year period exceeded $22,500, compared with $10,140 among non-headache sufferers. Similarly, the overall average pharmacy costs per eCH patient during this period were $8,200, which was nearly double that of the non-headache sufferers. Participants in surveys of sufferers indicate that CH is associated with a large socioeconomic burden. For
95
Table of Contents
example, research found that nearly 20% of patients with CH reported loss of employment and approximately 8% are unemployed or receiving disability services due to the disorder.
Other Therapies for Cluster Headache. Other than gammaCore, there is only one FDA-approved commercially available therapy for acute treatment for CH, injectable sumatriptan (Imitrex). The side effect profile and cost of Imitrex, however, typically limits patient access to only six to 10 doses per month, which usually enables patients to treat only a small fraction of their attacks each month. Even at this limited access level, the monthly cost of Imitrex for CH patients and their insurance providers averages more than $700. Imitrex use is also limited by the requirement for patients to subcutaneously self-inject, which may be particularly difficult to do while experiencing a CH attack. In a 2016 market research survey of CH patients, 87% of the respondents were dissatisfied with the then-available treatment options.
Preclinical Evidence of VNS Mechanisms of Action in Acute Cluster Headache
It is generally believed that the neural circuit involved in CH includes activation and inhibition of the trigeminal cervical complex, or TCC, shown in Figure 2 below. The TCC is a region of the brainstem associated with pain processing. Activation of facial nerves, including those relaying through the sphenopalatine ganglion, or SPG, activate the TCC. This belief is supported by evidence showing that activation of this pathway can cause CH-like attacks. Inhibition of the TCC is provided by inhibitory neurotransmitters, like serotonin, GABA and norepinephrine, which are released by neurons residing in the PAG, the NRM, and the locus coeruleus, or LC.
Figure 2: The neural circuit believed to be associated with CH.

(Figure adopted from S. Akerman and P. Goadsby, with permission)
One possible mechanism by which gammaCore acutely treats CH attacks may be through enhancement of inhibitory signals to the TCC. To test this, we sponsored research in which recording electrodes were inserted into the TCCs of rats to measure the effects of VNS on normal activity, or ongoing spontaneous neuronal firing, and activity under pain-simulated conditions, or dural-evoked pain fiber firing, the latter being caused by irritation of the outermost covering of the brain, or dura. As seen in the published graphs in Figures 3 and 4 below, VNS significantly suppressed activity in the TCC in both cases. These data suggest that the strengthening of the inhibition pathways is a mechanism of action for gammaCore.
96
Table of Contents
Figure 3: VNS applied in two doses, separated by five minutes, was able to suppress ongoing spontaneous firing of the neurons in the TCC, by more than 50%, with a duration of effect greater than two hours.

Figure 4: A pair of VNS doses, separated by five minutes was able to suppress firing of the pain fibers in the TCC under pain simulated conditions by approximately 30%, with a stable duration of effect of more than two hours.

Clinical Data of gammaCore as an Acute Treatment for Cluster Headache
We have completed one pilot trial and two parallel pivotal trials examining the efficacy, safety and tolerability of gammaCore for the acute treatment of CH as summarized in Table 2 below:
97
Table of Contents
Table 2: Overview of our CH trials for gammaCore

Our First Open-Label Trial
We sponsored an open-label trial of gammaCore for the acute treatment and prevention of CH at the Royal Free Hospital, published in 2015. The trial enrolled 25 patients, 19 of whom provided evaluable data. Of these evaluable patients, 11 had cCH and 8 had eCH. Seven of the cCH patients were considered to be drug-refractory and had failed reasonable attempts with multiple different preventative agents. Five patients with cCH provided long-term data for a full 52 weeks. In this trial, an evaluation of the efficacy of the therapy was based on patient-reported estimates of their CH attack frequency.
Fifteen of the 19 evaluable patients in this trial reported an overall improvement in their condition from baseline, with four stating that their condition had remained the same. No patients reported a worsening of their preexisting condition. Results demonstrated a mean improvement of 48% in CH attack frequency. Five of the eleven cCH patients had a one-year extended follow-up, which showed a mean estimated improvement in attack frequency at 26 weeks of 62% and maintenance at 52 weeks of 58%. In regard to acute efficacy, patients in this trial reported that gammaCore aborted attacks within an average time of 11 minutes of initial treatment. The long-term durability of this response was stable in four of the five patients with cCH who reported on their gammaCore use at both 26 and 52 weeks.
No serious adverse events were reported in this trial during and after treatment. Adverse events of mild severity reported in this trial included local discomfort during and after device use and mild skin reactions to the conductive gel.
Our Registration Trials for Acute Treatment of CH – ACT 1 and ACT 2
Our first FDA clearance, received following the grant of our de novo application, was for the acute treatment of eCH, and is supported by two multi-center, randomized clinical studies, ACT 1 and ACT 2. These trials, in aggregate, enrolled 253 patients, including both eCH and cCH patients. The primary endpoints of these trials were pain reduction and pain freedom within 15 minutes of the onset of the attack, i.e. mild pain or pain-free in ACT 1 and pain-free in ACT 2. Neither trial reached statistical significance with respect to the primary endpoint in the total population, but they did reach statistical significance on the primary endpoint and multiple secondary endpoints in their eCH subpopulation. eCH represents 80-90% of the overall CH population. In ACT 1, our gammaCore therapy demonstrated an ability to reduce pain to mild or pain-free status in eCH patients within 15 minutes of the onset of the attack more than three times as frequently as the sham treatment (gammaCore, 34.2%; sham, 10.6%; p<0.01). In ACT 2, which had a more stringent primary endpoint, our gammaCore therapy demonstrated an even stronger therapeutic effect compared to the sham treatment among eCH patients (gammaCore, 47.5%; sham, 6.2%; p<0.01).
98
Table of Contents
Our ACT 1 Trial – gammaCore for the Acute Treatment of Episodic and Chronic Cluster Headache
ACT 1 was a pivotal, randomized, double-blind, sham-controlled prospective trial of gammaCore for the acute treatment of CH. The trial enrolled 150 patients and was conducted at 20 centers in the United States, including academic medical centers and other tertiary headache clinics. ACT 1 was designed to assess the superiority of our gammaCore therapy in comparison to sham treatment and was comprised of two phases: (1) a double-blind phase in which patients were randomized to receive gammaCore therapy or sham treatment for one month or until five CH attacks were treated and (2) an open-label phase in which patients who completed the double-blind phase could subsequently receive three months of our gammaCore therapy. The primary endpoint for the trial was response rate, defined as the proportion of patients who achieved pain relief (pain intensity of 0 or 1 on a 5 point scale) at 15 minutes after treatment initiation for the first CH attack treated. Investigators, patients, and study coordinators were blinded to treatment assignments in the double-blind phase of the trial. The ACT 1 results were published in 2016.
Figure 5: ACT 1 Trial Consort Diagram

As shown in Figure 5 above, in ACT 1, 150 patients were enrolled and 133 patients met the criteria for the intent-to-treat, or ITT, population (gammaCore, n=60; sham, n=73). Of the 133 patients in the ITT population, 128 patients entered the open-label period, 100 of whom completed the trial. Twenty-eight patients did not complete the open-label period for a variety of reasons, the most common of which was persistence of their CH condition during the treatment period. Demographic and baseline characteristics were similar between the gammaCore and sham cohorts and were consistent with those of a typical CH population. Of the 133 patients in the ITT cohort, most had eCH (85) and the remaining had cCH (48).
Response rates for the primary endpoint in the total ITT population, which includes both eCH and cCH patients, were numerically superior for gammaCore than for sham treatment (gammaCore, 26.7%; sham, 15.1%; p=0.1). Additionally, as shown in Figure 6 below, in a predefined analysis of the eCH subpopulation, a significantly higher response rate was demonstrated with gammaCore than with sham (gammaCore, 34.2%; sham, 10.6%; p<0.01).
99
Table of Contents
Superior sustained treatment response rates were statistically significant for gammaCore compared with sham among the total population (gammaCore, 26.7%; sham, 12.3%; p=0.04), however, this superior response was most pronounced for the eCH subpopulation (gammaCore, 34.2%; sham, 10.6%; p<0.01). This observation of strongest clinical benefit in the eCH cohort was also demonstrated with respect to the proportion of patients who were responders at 15 minutes for ³50% of their treated attacks (gammaCore, 34.2%; sham, 14.9%; p=0.04). Results were also significant in the eCH subpopulation for the proportion of those who were pain-free at 15 minutes for ³50% of treated attacks (gammaCore, 15.8%; sham, 2.1%; p=0.04).
Figure 6: Selected Results for eCH Patients in the ACT 1 Trial

No serious adverse events, or SAEs, were attributable to gammaCore in ACT 1. Across all patients, 33% (49/150) had one or more adverse events, or AEs, during the double-blind period (gammaCore, 18; sham, 31). AEs occurred in 35 patients during the double-blind phase, at more than double the rate in the sham cohort than the gammaCore subpopulation. During the open-label period, 33% (42/128) of all patients had one or more AEs. As shown in Table 3 below, the most commonly occurring adverse events relating to the therapy, or ADEs, were application site reactions, all of which were mild, transient, and tended to be self-limiting in nature.
Table 3: Most Commonly Reported ADEs from the ACT 1 Trial

100
Table of Contents
ACT 1 was the first randomized, double-blind, sham-controlled trial evaluating the effects of non-invasive neuromodulation for the acute treatment of CH. As seen in the pre-defined subpopulation analysis, gammaCore demonstrated significant therapeutic benefit across a broad range of endpoints for the eCH subpopulation, including first attack response rate, sustained treatment response rate, the percentage of patients who responded to gammaCore for ³50% of their attacks, and of those, the percentage who were pain-free. These results suggest that response to an initial gammaCore treatment predicts likely response to treatment for subsequent attacks. In addition, among the full study population, the average duration of attack for the first attack treated was reduced among the gammaCore-treated cohort by an average of 9.5 minutes while the sham-treated group reported an attack duration that increased by 12.8 minutes. This difference was statistically significant (p=0.03). Among the eCH subpopulation, this difference was more pronounced, with the gammaCore group experiencing an average decrease in attack duration of 14.4 minutes, while the sham-treated group reported their average attack duration rise by 16.3 minutes (p=0.03). Attack duration has not traditionally been used to quantify clinical meaningfulness of treatments in CH, however, given the extreme nature of the pain associated with these attacks, it is further support for the value of our gammaCore therapy, especially among eCH patients.
Our ACT 2 Trial – gammaCore for the Acute Treatment of Episodic and Chronic Cluster Headache
ACT 2 was a pivotal, randomized, double-blind, sham-controlled prospective trial of gammaCore for the acute treatment of eCH and cCH. The trial enrolled 103 patients and was conducted in four European countries at academic medical centers and other tertiary headache clinics. ACT 2 was designed to assess the superiority of our gammaCore therapy in comparison to sham treatment and was comprised of three phases: (1) a one-week run-in period, (2) a two-week, randomized, double-blind period during which patients were treated with either our gammaCore or sham therapy, and (3) a two-week, open-label period in which patients could subsequently receive gammaCore therapy. The primary endpoint for the trial was response rate, defined as the proportion of all attacks that achieved pain freedom at 15 minutes after treatment initiation. Investigators, patients, and trial coordinators were blinded to treatment assignments during the double-blind period. In total, 495 attacks were treated with active gammaCore therapy and 400 with the sham treatment. The ACT 2 trial results were published in 2017.
101
Table of Contents
Figure 7: ACT 2 Trial Consort Diagram

As shown in Figure 7 above, in ACT 2, 103 patients were enrolled, 102 patients met the criteria for the safety population, and 92 patients met the criteria for the ITT population (gammaCore, n=48; sham, n=44). Of the 92 patients in the randomized phase of our ACT 2 trial, 83 entered the open-label period and 79 completed the trial. Demographic and baseline characteristics were similar between the gammaCore and sham cohorts and were consistent with those of a typical CH population. Of all 102 patients in the safety population, most had cCH (71%) and the remaining 29% had eCH. Although eCH occurs more frequently than cCH, we enrolled more cCH patients in the ACT 2 trial because a greater proportion of them are in bout at any given time.
Figure 8: Selected Results for predefined eCH subpopulation in the ACT 2 Trial

102
Table of Contents
As shown in Figure 8 above, consistent with the results from the ACT 1 trial, a predefined subpopulation analysis in ACT 2 demonstrated a higher response rate to gammaCore in the eCH subpopulation than in the cCH subpopulation. In the eCH subpopulation, a higher proportion of treated attacks achieved pain-free status with gammaCore than with sham (gammaCore, 47.5%; sham, 6.2%; p<0.01). No treatment difference for this endpoint was seen in the cCH cohort (gammaCore, 4.8%; sham, 12.9%; p=0.13) in this trial.
The mean proportion of treated attacks per subject that achieved responder status within 30 minutes was greater with gammaCore than with sham for the total ITT population (gammaCore, 42.7%; sham, 27.6%; p=0.05).
As shown in Table 4 below, the proportion of subjects who achieved responder status with statistical significance for ³50% of treated attacks at 15 minutes was higher with gammaCore than with sham in the total ITT population (gammaCore, 39.6%; sham, 13.6%; p<0.01) and the eCH subpopulation (gammaCore, 64.3%; sham, 15.4%; p<0.01), but was not higher with statistical significance in the cCH cohort (gammaCore, 29.4%; sham, 12.9%; p=0.11).
Table 4: Selected Results for the ACT 2 Trial

No SAEs were attributable to gammaCore in ACT 2. Of all patients, 33% (34/102) had one or more AEs during the double-blind phase of the trial. Of the non-serious AEs, 19 patients (gammaCore, 9; sham, 10) experienced one or more treatment-related AEs during the double-blind phase of the trial. As shown in Table 5 below, the most commonly occurring of these AEs were application site reactions, all of which were mild, transient, and tended to be self-limiting in nature.
Table 5: Most Commonly Reported ADEs from the ACT 2 Trial

The ACT 2 trial results confirm and extend the findings from ACT 1. ACT 2 demonstrated the significant therapeutic benefit of gammaCore across a broad range of endpoints, including the mean proportion of treated attacks per subject that achieved responder status within 15 minutes across all patients. The greatest clinical benefit was observed in a predefined analysis of the eCH subpopulation, including the proportion of all treated attacks that achieved pain-free status within 15 minutes and 30 minutes. These results suggest that initial response to our gammaCore therapy predicts likely response to treatment for subsequent attacks. As with our ACT 1 trial, gammaCore was well tolerated in ACT 2.
103
Table of Contents
Our Pooled Analysis of ACT1 and ACT2 for the Acute Treatment of Episodic Cluster Headache
To further define the benefit of gammaCore for the acute treatment of eCH, the data from ACT 1 and ACT 2 were pooled to assess the overall response to each trial’s primary endpoint, as shown in Figure 9 below. Collectively there were 112 eCH patients and 113 cCH in the pooled data set. Among the 112 patients with eCH, more patients who treated with gammaCore achieved mild or pain-free status at 15 minutes for the first attack treated (the ACT1 primary endpoint) compared with those in the sham cohort (gammaCore, 38.5%; sham, 11.7%; p<0.01). Similarly, the proportion of all treated attacks in these eCH subpopulation reaching pain freedom at 15 minutes (the ACT 2 primary endpoint) was greater in the gammaCore cohort compared to the sham cohort (gammaCore, 24.1%; sham, 7.3%; p<0.01). Both studies individually met statistical significance on this endpoint (ACT 1: gammaCore, 15%; sham, 6%; p<0.05; ACT 2: gammaCore, 48%; sham, 6%; p<0.05).
The proportion of these eCH patients who achieved mild or pain-free status at 15 minutes in ³50% of their treated attacks was higher for gammaCore compared to sham (gammaCore, 42.3%; sham, 15.0%; p=0.01). These findings are consistent with the findings of each trial individually (ACT 1: gammaCore, 34.2%; sham, 14.9%; p=0.04; ACT 2: gammaCore, 64.3%; sham, 15.4%; p=0.02).
Figure 9: Selected Results of the Pooled Analysis of the ACT 1 and ACT 2 Trials for eCH Patients

This analysis demonstrated that gammaCore is effective and well tolerated in aborting attacks in eCH, but did not appear to have similar efficacy in cCH. Important advantages over existing treatment options are that gammaCore is easy-to-use and may be applied for as many attacks as a patient experiences per day, without the frequency-of-use restrictions and contraindications associated with other treatments.
Migraine
The Condition. Migraine is a debilitating condition characterized by severe throbbing pain usually on one side of the head, often associated with nausea and sensitivity to light and sound. The pain associated with migraine attacks often has a pulsing quality that is synchronized with heartbeat and is typically worsened by physical activity. According to the International Classification of Headache Disorders, the pain phase of a migraine can last for four to 72 hours. More than two-thirds of sufferers are unable to work or function normally during the pain phase of a migraine attack.
Migraine attacks are characterized by the presence or absence of a preceding aura phase. Aura is a phenomenon associated with neural hyperactivation and synchronized depolarization in the brain, and is
104
Table of Contents
characterized by visual or other functional disturbances. 30% of patients report aura preceding at least a portion of the migraine attacks they experience. Migraines are categorized by the frequency with which they occur. With chronic migraine, affecting 10% of the total migraine population, patients suffer migraine attacks on 15 or more days of the month, on average. With episodic migraine, patients experience 14 or fewer migraine attacks per month.
Prevalence and Market Size. According to the World Health Organization, migraine ranks as the third most common disease in the world and the leading cause of disability among neurological disorders. Migraine will affect approximately 12% of the adult population globally, currently affecting approximately 36 million people in the United States, the majority of whom are women of childbearing years. Population-based studies of insured individuals reveal that, annually, 4.5% of the adult population seeks treatment for primary headache, the vast majority of which is for migraine. In the United States and EU, research has found that the age of first diagnosis of migraine peaks in the early-to-mid teens and the disease continues to persist throughout adulthood for many of these sufferers, demonstrating that it is often a disorder of long duration.
An estimated five million migraine patients in the United States require the care of a headache specialist. These specialists, many of whom also treat CH, comprise the approximately 1,100 physicians who practice in over 120 tertiary care centers in the United States. Although the triptan drug class is the current standard of care for the acute treatment of migraine, according to the U.S. Pharmacist, a leading pharmacy publication, more than 60% of patients have reported dissatisfaction with, or have contraindications to, the current standard of care, such as triptan medications. This dissatisfaction may partly explain the sub-25% penetration rate for available generic triptan medications. Despite these limitations, we estimate that the addressable market for the acute treatment of migraine in the United States in 2018 will be approximately $3.8 billion.
Economic Burden. Over the past several decades, migraine has been associated with persistently greater total annual medical costs. An independent study conducted in 1999 found that migraine sufferers in California had annual total medical expenses two and a half times higher than non-migraine sufferers. A 2011 study conducted by GNS Healthcare and sponsored by us demonstrated consistent results among the nearly 5% of 21 million privately insured patients in the United States who receive diagnosis of migraine annually.
Current Acute Migraine Treatments and Their Limitations. Triptan medications, or Triptans, are a family of tryptamine-based drugs first sold in the 1990s, which account for approximately 80% of the acute treatments prescribed for migraine. Triptans are sold in oral, nasal, and subcutaneous formulations. Through their binding to specific seratonin receptor subgroups, Triptans cause constriction of blood vessels in the outer covering of the brain, or the meninges. This vasoconstrictive activity also affects blood vessels in other areas of the body, including the heart, which accounts for important risks associated with their use, and labeling limitations on the frequency of their use.
Other less commonly prescribed acute migraine treatments include ergotamines and analgesics, including non-steroidal anti-inflammatory drugs, or NSAIDs, acetaminophen and antiemetics. Dihydroergotamine, or DHE, is a grain fungus derivative that, like triptans, is a potent vasoconstrictor. DHE has been used for more than 50 years for the treatment of migraine, but modern physicians rarely prescribe it because of significant side effects. More specifically, ergotamines and triptans are both vasoconstrictors with labels citing the risk of their use in migraine sufferers with risk factors for cardiovascular disease.
Opioids are often dispensed for migraine attacks in emergency departments; however, in the treatment guidelines referenced by the National Institutes of Health, their use is not recommended for the acute treatment of migraine. Opioid use for migraine is associated with increased disability and health care utilization. The U.S. Centers for Disease Control and Prevention has recognized the growing issue of
105
Table of Contents
opioid misuse, abuse and addiction and officially classified prescription opioid abuse as an epidemic. Data from a 2009 study conducted by the American Migraine Prevalence and Prevention Study suggests that about 16% of migraine patients are current opioid users and 16% of those patients are likely dependent.
Preclinical Evidence of nVNS Mechanism of Action in Acute Migraine
Although the cause of migraine is multifactorial, one validated model, shown in Figure 10 below, involves the activation of nerve fibers in the dura through a mechanism similar to the one previously described for CH. These fibers lie in close proximity to blood vessels passing through the dura, and connect through the trigeminal ganglion to the TCC. Excessive firing of the TCC involves the increased release of the excitatory neurotransmitter glutamate and is associated with migrainous pain. As in the case of CH, this activation is typically opposed by the release of inhibitory neurotransmitters, including serotonin, norepinephrine, and GABA. Migraine pain may be experienced when excessive firing from the TCC exceeds the inhibitory mechanisms, or if the inhibitory mechanisms are not present.
Figure 10: The neural circuit believed to be associated with migraine

(Figure adapted from S. Akerman and P. Goadsby, with permission)
To show the effects of nVNS, we sponsored a preclinical study at Thomas Jefferson University, published in 2014. In this study, animals were sensitized, rendering them allodynic, or sensitive to touch, and susceptible to increased pain when the known migraine trigger, nitroglycerine, or GTN, was administered. Previous research had shown significant increases in glutamate expression in the TCC, specifically in the trigeminal nucleus caudalis from GTN exposure. The results of our study, provided in Figures 11 and 12 below, showed that administration of nVNS simultaneously with, or 90 minutes after GTN was administered, reduced both the pain behavior and the over-expression of glutamate.
106
Table of Contents
Figure 11: Co-administered nVNS prevents the significant increase in glutamate expression triggered by GTN in sensitized animals.

Figure 12: Administration of nVNS, 90 minutes after GTN reduces over-expression of glutamate that occurs in sensitized animals.

The pulsating character of migraine pain supports the inference of a relationship between activated nerve fibers and blood vessels that are in close proximity with one another. This pulsating feature, typically exacerbated by exercise, led early observers to suspect vasodilation as an underlying cause. As previously mentioned, triptans, which are vasoconstrictors, are the most widely prescribed medications for the acute treatment of migraine. Further, over the past decade, research in headache has included a focus on calcitonin gene-related peptide, or CGRP, which is a peptide released by neurons under a variety of stress conditions. CGRP is the most potent, endogenously produced vasodilator. The administration of exogenous CGRP in sensitized animals and human migraineurs has been shown to trigger pain-related behavior and migraines.
Models of CGRP activity in migraine suggest that neurons releasing CGRP in the TCC result in the activation of pain pathway neurons, leading to acute headache pain. While several stresses can cause the release of CGRP, the inflammatory cytokine tumor necrosis factor alpha, or TNF-a, is known to trigger its synthesis and release from neurons. Heightened expression of TNF-a has been correlated with heightened expression of CGRP as well as its receptors. As previously mentioned, published results of multiple studies show that VNS is capable of suppressing TNF-a in the central nervous system.
107
Table of Contents
To further study the effects of our gammaCore therapy in migraine, and specifically as it relates to CGRP, we sponsored a series of studies in which animals were sensitized by chronic inflammation. These animals experience migraine-like pain upon exposure to a known migraine trigger, umbellulone. The results of this study, as shown in Figure 13 below, demonstrated that nVNS reduces pain responses of sensitized animals relative to that of naïve animals, whether the therapy is delivered before or after the trigger is administered.
Figure 13: Administration of nVNS after umbellulone exposure reduces pain-associated behavior in inflammation-sensitized animals.

In addition to the reduction in pain, nVNS reduced the expression of intracellular biomarkers of inflammation. These biomarkers are associated with an upregulation in TNF-a, and correspondingly, in CGRP synthesis and expression.
Clinical Data in support of gammaCore for Acute Migraine Treatment
We have completed one pilot and one pivotal trial examining the efficacy, safety and tolerability of gammaCore for the acute treatment of migraine headache as summarized in Table 6 below:
Table 6: Overview of Our Acute Migraine Trials for gammaCore

Our First Open Label Trial in Acute Migraine
We sponsored a multi-center, pilot clinical trial to investigate the use of gammaCore for the acute treatment of migraine headache, published in 2014. The trial was an open-label, single-arm, multiple-attack trial conducted at four headache centers in the United States. Patients were asked to treat up to four acute migraine attacks with gammaCore over a six week period. The trial enrolled 30 patients, 25 of whom were female and 27 of whom treated at least one attack.
108
Table of Contents
Nineteen of the 27 patients treated their first attack at a pain level that was moderate or severe at baseline. Four of these 19 patients (21%) reported being pain free at two hours. Nine of 19 patients (47%) reported pain relief, defined as mild pain or pain free, at the same time point. The eight remaining patients treated their first attack while at mild pain at baseline, five of whom (63%) were pain free at two hours. Overall, these 27 patients treated 80 migraines, 54 of which were treated with a baseline pain level of moderate or severe. Twelve of 54 attacks (22%) were reported as pain free at two hours, and 23 of 54 attacks (43%) reached pain relief. The remaining 26 attacks were treated at mild pain, and pain freedom was achieved for 10 of these attacks (38%). The efficacy results from this trial are similar to other acute treatments for migraine.
This pilot trial demonstrated gammaCore is well tolerated in patients with acute migraine. Adverse events were of mild severity, transient in duration, and included local discomfort during and after gammaCore use, as well as mild skin reactions to the conductive gel. Based on the results of this trial, the authors noted that gammaCore seemed better tolerated than triptan medications and did not appear to have the cardiovascular or cerebrovascular risks associated with them.
The PRESTO Trial – Our Registration Trial for the Acute Treatment of Migraine
Our PRESTO trial, or PRESTO, was a pivotal, randomized, double-blind, sham-controlled prospective trial of gammaCore for the acute treatment of migraine. The trial enrolled 285 patients and was conducted at 10 centers in Italy, including academic medical centers and other tertiary headache clinics. PRESTO was designed to assess the superiority of our gammaCore therapy in comparison to sham treatment and included three four-week periods: (1) a run-in period; (2) a double-blind period; and (3) an open-label period. Patients treated up to five migraine attacks with gammaCore or sham in the double-blind period and up to five additional attacks with gammaCore in the open-label period. The primary endpoint for the trial was response rate, defined as the proportion of patients who achieved pain freedom at 120 minutes after treatment initiation for the first migraine treated. Investigators, patients, and study coordinators were blinded to treatment assignments in the double blind phase of the trial.
Figure 14: PRESTO Trial Consort Diagram

109
Table of Contents
As shown in Figure 14 above, 285 patients were enrolled into the run-in period of PRESTO, 248 of whom were eligible for randomization into the double-blind period. 37 patients did not randomize, the majority of whom failed to meet the entry criteria for randomization. 243 of the 248 enrolled patients treated at least one attack and represent the ITT population (gammaCore, n=120; sham, n=123). Of the ITT population, 239 entered the open label period, and 238 finished the open label period. Demographic and baseline characteristics were generally well balanced between the gammaCore and sham cohorts, however, clinically relevant trends were observed with respect to preventative medication use and pain level at baseline. A higher proportion of patients in the gammaCore cohort treated their first attack when its intensity was severe.
As shown in Figure 15 below, the proportion of patients in the gammaCore cohort who became pain-free after treating the first attack was significantly higher than those who treated with sham at 30 minutes (gammaCore, 12.7%; sham, 4.2%; p=0.01) and 60 minutes (gammaCore, 21.0%; sham, 10.0%; p=0.02) but not at 120 minutes (gammaCore, 30.4%; sham, 19.7%; p=0.07; primary endpoint). A repeated-measures test, recommended by our independent statisticians, examined the inconsistency between the 120-minute finding and the 30- and 60-minute findings and demonstrated the statistical significance of gammaCore’s superiority over sham for the pain-free outcome through 120 minutes (odds ratio: 2.3; 95% CI: 1.2, 4.4; p=0.01).
Figure 15: Primary Endpoint and Repeated Measures Analysis of the PRESTO Trial for Acute Migraine

As shown in Figure 16 below, the proportion of patients who achieved pain relief, defined as mild or no pain, at 120 minutes was significantly higher with gammaCore than with sham for the first treated migraine attack (gammaCore, 40.8%; sham, 27.6%; p=0.03). The proportion of patients who responded at 120 minutes for ³50% of their attacks was significantly higher with gammaCore than with sham for both pain freedom (gammaCore, 32.4%; sham, 18.2%; p=0.02) and pain relief (gammaCore, 47.6%; sham, 32.3%; p=0.03).
110
Table of Contents
Figure 16: Selected Secondary and Exploratory Results of the PRESTO Trial for Acute Migraine

As shown in Figure 17 below, mean percentage pain reduction for the first attack was significantly greater with gammaCore than with sham at 60 minutes (gammaCore, -25.4%; sham, -7.7%; p=0.03) and 120 minutes (gammaCore, -34.8%; sham, -5.4%; p<0.01).
Figure 17: Percent Pain Relief Results of the PRESTO Trial for Acute Migraine

No SAEs were attributable to gammaCore in PRESTO. Of all patients, 18% (45/248) had ³1 AE during the trial. As shown in Table 7 below, the most commonly occurring device-related AEs of these were application site reactions, all of which were mild, transient, and tended to be self-limiting in nature. The PRESTO trial demonstrated gammaCore to have a highly favorable tolerability profile.
111
Table of Contents
Table 7: Most Commonly Reported Device-Related ADEs from the PRESTO Trial

Headache Prevention
The grant by FDA of our de novo application resulted in a new Class II regulatory category: external vagal nerve stimulator for headache. The establishment of this product category permits us to apply for label expansions through the 510(k) regulatory pathway utilizing our own product as the predicate. It is our intention to seek the expansion of our label for the prevention of both migraine and eCH. As described below, we have run, and continue to conduct, additional clinical studies which may support label expansion for the acute treatment and prevention of other primary and secondary headaches.
Cluster Headache Prevention
As described previously, CH is believed to be the result of stimuli from facial nerves that activate the TCC, and which are opposed by inhibitory neurotransmitters from key areas of the brainstem. Acute activation of these inhibitory mechanisms has been proposed as the basis for gammaCore’s clinical efficacy in the treatment of CH attacks. The clustering of these attacks suggests a prolonged susceptibility of CH patients to loss of inhibition, or excessive activation. Prevention, therefore, may be possible by reducing the susceptibility of the circuit either by sustained elevation of baseline inhibition, or elimination of the stimuli activating the facial nerves.
In one model of CH, prolonged irritation of the facial tissue, which includes the sinus passages around the orbital socket, may cause activation of the facial nerves. Periodic inflammation of the sinuses may be related to the observed increase in episodic CH activity in the spring and fall, when allergens are more prevalent. Consistent with this mechanism, corticosteroids, like prednisone, have shown efficacy as a preventative treatment for patients entering a cluster bout. Unfortunately, because of the side effects of prolonged steroid use, steroids are typically only prescribed in short duration.
Currently Used Therapies for Cluster Headache Prevention and Their Limitations. There are currently no FDA approved medications for the prevention of CH, driving off-label use of medications, such as lithium, valproic acid and high-dose verapamil. These medications have unproven efficacy and the potential for significant health risks, including adverse cardiac events, organ toxicity and birth defects. As a result, patients are confronted with the difficult choice of continuing to suffer CH attacks unabated or to try treatments with uncertain clinical benefit and the potential for serious medical consequences.
Our PREVA Trial – gammaCore for Prevention and Acute Treatment of Chronic Cluster Headache
Our PREVA trial, or PREVA, was a prospective, multi-center, open-label, randomized, controlled, parallel-group trial of gammaCore for the prevention of cCH. The trial enrolled 114 patients with 97 patients randomized and was conducted at 10 sites in Europe, including academic medical centers and other tertiary headache clinics. PREVA was designed to assess the superiority of adjunctive use of our gammaCore therapy with standard of care medications in comparison to standard of care medication alone, and included three periods: (1) a two-week baseline phase during which all patients received only their individualized standard of care, or SoC, (2) a four-week randomized period during which
112
Table of Contents
participants were randomly assigned the adjunctive treatment or SoC arms; and (3) a four-week open label period during which all participants received adjunctive gammaCore therapy. The primary endpoint for the trial was defined as the mean change from baseline in the number of weekly attacks in the third and fourth week of the randomized period compared with the average weekly attack rate in the baseline period.
Figure 18: PREVA Trial Consort Diagram

As shown in Figure 18 above, in PREVA, 114 patients were enrolled and assessed at baseline, 97 of whom provided baseline data and were considered reliable trial participants. Of these patients, 93 met the criteria for inclusion in the ITT population having provided evaluable data (gammaCore, n=45; SoC, n=48). Of the ITT population, 92 provided data in the open-label period (gammaCore, n=44; SoC, n=48). Demographics and baseline characteristics were similar between these groups and were representative of the overall CH population. Use of SoC medications was also comparable between groups. A modified ITT, or mITT, population, defined to include only patients with measurable data across the respective study periods (gammaCore, 37/45; SoC, 47/48), was also provided in the primary publication of these data in 2016.
As shown in Figure 19 below, during the randomized period, participants receiving adjunctive gammaCore treatment had a significantly greater reduction from baseline in the number of CH attacks per week compared to those receiving SoC alone (gammaCore, -5.9; SoC, -2.1; p<0.02). In the mITT population, the therapeutic benefit was more pronounced in the adjunctive gammaCore cohort (gammaCore, -7.2; SoC, -2.1; p<0.001). To determine the efficacy of longer-term prophylactic use of gammaCore, the reduction in the number of CH attacks during the open label period was examined in the 30 patients who continued adjunctive gammaCore use through this period. These patients reported a statistically significant reduction of two CH attacks per week (p<0.001) compared with the randomized period, suggesting further benefit with continued adjunctive use of our therapy.
113
Table of Contents
Figure 19: Primary Endpoint Analysis of the ITT and mITT Populations for the PREVA Trial

As shown in Figure 20 below, in the ITT population, a significantly higher proportion of the patients receiving adjunctive gammaCore treatment experienced a ³50% reduction in CH attack frequency during the randomized period compared with the SoC cohort (gammaCore, 40.0%; SoC, 8.3%; p<0.001). Similarly, the response rate in the mITT population was also significantly higher for individuals receiving adjunctive gammaCore therapy (gammaCore, 48.6%; SoC, 8.5%; p<0.001), suggesting that patients who remained in the trial had greater response.
Figure 20: Responder Rate Analysis for the ITT and mITT Populations in the PREVA Trial

The use of abortive medications to acutely treat CH attacks was reported during all three periods of the trial. Changes in the use of acute medication are generally used as a surrogate for efficacy in preventing the occurrence of CH attacks. Reliable data on the use of abortive medications was only available in the mITT population. The number of times abortive medications were used in this population during the last two weeks of each trial period is shown in Figure 21 below. During the randomized period, the gammaCore cohort reported a statistically significant decrease of 61.1% (p<0.01) in the frequency of use of subcutaneous sumatriptan injections over the baseline period, whereas the SoC cohort reported an
114
Table of Contents
10.3% increase in the use of this injected medication over baseline. Changes in the use of high-flow oxygen showed a similar difference in favor of adjunctive gammaCore use in that the reduction in its use among the gammaCore cohort was 62.4% (p=0.02) compared with only a 14.3% reduction in the SoC cohort. Similar results were seen in the open-label period.
Figure 21: Change in Abortive Medication Use for the mITT Population in the PREVA Trial

In our PREVA trial, no SAEs were attributable to gammaCore. During the two months of treatment, similar proportions of participants in the gammaCore cohort and SoC cohort (gammaCore, 52%; SoC, 49%) reported AEs. Most AEs were mild or moderate (93% (108/116)). Overall, as shown in Table 8 below, the most common AEs were CH attacks (gammaCore, 1; SoC, 5), along with nasopharyngitis, dizziness, oropharyngeal pain, and neck pain.
Table 8: Most Commonly Reported AEs from the PREVA Trial

In summary, this trial met its primary endpoint by demonstrating that daily adjunctive prophylactic use of our gammaCore therapy significantly reduced the number of CH attacks per week, which led to substantial reductions in abortive medication use.
Prevention of Migraine
At sufficient exposure, migraine triggers such as lack of sleep, low oxygen levels and toxins, like alcohol, are capable of causing headaches. Some individuals experience migraine attacks after modest exposure to
115
Table of Contents
these and other triggers. When identifiable, avoidance of such triggers is a staple technique for migraine prevention.
Despite trigger identification and employment of a corresponding avoidance strategy, there remains a high unmet need among migraineurs for safe and effective preventative therapies. According to the U.S. Agency for Healthcare Research and Quality, only about 12% of adults with high frequency or chronic migraine take preventive medications. According to the American Migraine Foundation, medication side effects often limit the use of migraine medications.
Currently Used Therapies for Migraine Prevention and Their Limitations. Five products are currently approved by the FDA for the prevention of migraine: anti-epileptic drugs, topiramate (Topamax) and valproic acid (Depakote), beta-blockers, propranolol (Inderal) and timolol (Blocadren), and BOTOX. BOTOX is the only product that has been approved by the FDA for the prevention of chronic migraine, and its label is limited to that subgroup. In all cases, these medications were first approved for other uses.
These current treatments are ineffective or inconvenient for many patients, and their use has been limited by issues with tolerability and side effects, including cognitive impairment, nausea, fatigue and sleep disturbance. Anti-epileptic drugs are also associated with poor pregnancy outcomes and fetal abnormalities, which is a concern for women of childbearing years. In clinical trials, these medications require four to six weeks of daily administration before most patients experience measurable clinical benefit. For example, BOTOX requires approximately 31 subcutaneous injections at various sites on the head and neck, repeated every 12 weeks.
We believe there is a need for a new therapy that can either prevent migraines or reduce their severity to a level at which supplemental existing abortive therapies can provide relief as needed, with reduced side effects. Such a therapy could provide benefit for both patients on existing therapies and patients who have abandoned therapy.
Mechanisms of Action Evidence Supporting gammaCore Use in Migraine Prevention
Approximately 25% of all migraine patients experience sensory symptoms known as “aura” prior to the pain stage of at least a portion of their migraine attacks. Aura is characterized by visual symptoms, most frequently, or by other symptoms associated with synchronized depolarization in the brain. This synchronized depolarization, referred to as cortical spreading depression, or CSD, is believed to occur more readily when the brain is in a hyperexcitability state. Based on their ability to reduce brain hyperexcitability, several anti-epileptic drugs are used for the prevention of migraine.
To investigate the effects of VNS, which was first used clinically in epilepsy, on hyperexcitability, we sponsored a series of pre-clinical studies at the Massachusetts General Hospital. The results, published in 2016, showed that our gammaCore therapy rapidly increased the thresholds for triggering CSDs, and reduced brain hyperexcitability. In contrast to the chemical medications mentioned above, a two-minute dose of our therapy was able to multiply by approximately 2.5 times the intensity of the trigger required to initiate CSDs within 20 minutes of initial treatment. This compares favorably to drug treatments that require weeks to months of daily administration, often with associated side effects, before achieving clinical benefit.
Recently published genetic and epigenetic studies suggest a strong association between migraine and genes tied to severe inflammatory conditions. These findings, coupled with recent breakthroughs in our understanding of how the immune system affects the expression of neurotransmitters, CGRP, and their receptors, may enhance our explanations of how hyperexcitability arises. To further this understanding, we sponsored studies in which prolonged inflammation was used to sensitize animals to respond to migraine triggers.
116
Table of Contents
In this work, twice-daily gammaCore treatments, administered during the prolonged inflammation period, inhibited sensitization. Animals treated with gammaCore were indistinguishable from a non-sensitized animal group in their lack of response to the migraine trigger, which contrasted with the sensitized group not treated with gammaCore, which responded with pain behavior. Brainstem tissue from the untreated, sensitized group was analyzed, and showed evidence of CGRP synthesis, as well as a greater number of actual CGRP vesicles. In contrast, both non-sensitized animals and gammaCore-treated animals exhibit normal intracellular biomarkers of CGRP synthesis and normal levels of CGRP vesicles. Further tissue analysis revealed that pain pathway neurons in sensitized animals exhibited elevated expression levels of CGRP receptors. In contrast, the non-sensitized and the gammaCore-treated animals showed no elevation in CGRP receptor populations.
We believe these preclinical studies provide mechanistic support for the development of gammaCore for the prevention of migraine.
Clinical Data in Support of gammaCore for Migraine Prevention
Our EVENT Trial – Chronic Migraine Headache Prevention with gammaCore
Our EVENT trial was a multi-center, randomized, sham-controlled pilot clinical trial with respect to the use of our gammaCore therapy for the prevention of chronic migraine and was published in 2016. This prospective double-blind pilot trial was conducted at six tertiary care headache centers in the United States. The trial included three consecutive periods: (1) a one-month baseline period during which patients provided data regarding their frequency of headache attacks to serve as a baseline comparator; (2) a two-month, randomized, sham-controlled period during which patients received prophylactic treatment with gammaCore or a sham; and (3) a six-month open-label period during which all patients received gammaCore. The primary objective of the EVENT trial was to assess the feasibility, safety, and tolerability of our gammaCore therapy, and as such, was not powered to reach statistical significance with respect to any efficacy measures. The trial enrolled 59 patients.
At baseline, the mean number of headache days in the gammaCore cohort (n=30) was 20.8 and 22.0 for the sham cohort (n=29). At the conclusion of the randomized period, the gammaCore cohort had experienced an average reduction of 1.4 migraine days while the sham cohort experienced a 0.2 migraine day decrease. The mean change from baseline was not statistically significant between groups. A per protocol cohort was identified in whom the mean migraine day reductions for the gammaCore and sham cohorts were 2.0 and 0.1, respectively.
During the open-label period, the original gammaCore cohort experienced continued reductions in migraine days. In this period, patients in the sham cohort gained access to gammaCore and began to show improvement. The data from this trial demonstrated that continued use of our gammaCore therapy provides increased benefit. A post hoc completers analysis demonstrated statistically significant and clinically meaningful reductions from baseline at the conclusion of the trial in both cohorts (initial gammaCore randomization cohort, 8.0 migraine-day reduction; initial sham randomization cohort, 6.0).
The primary purpose of this trial was safety and tolerability. Our gammaCore therapy was well tolerated and mild to moderate adverse events were generally similar in both groups.
The PREMIUM Trial – Our Registration Trial for the Prevention of Migraine
Our PREMIUM trial, or PREMIUM, is a pivotal, randomized, double-blind, sham-controlled prospective trial of gammaCore for the prevention of migraine. The trial is being conducted at 22 centers in Europe, included academic medical centers and other tertiary headache clinics, and enrolled 477 patients into a 28-day baseline run-in period, 341 of whom are included in the safety population and 332 of whom are included in the ITT population. PREMIUM was designed to assess the superiority of our gammaCore
117
Table of Contents
therapy in comparison to sham treatment and included three distinct periods: (1) a 28-day run-in period; (2) a three-month double-blind period; and (3) a six-month open-label period. PREMIUM has progressed through the randomized period and is currently in the open-label period. The data presented herein below relate to the randomized period only and are the result of preliminary analytics performed by our independent third-party statisticians. Patients were instructed to treat themselves with two 120-second doses of gammaCore therapy or sham treatment, twice per day. Patients randomized to the sham treatment were offered the opportunity to use gammaCore during the open-label period. The primary endpoint for the trial is a reduction in the average number of migraine days per month during the third month of the randomized period compared to the average number of migraine days per month in the baseline period between the two cohorts. Investigators, patients, and study coordinators were blinded to treatment assignments in the double blind phase of the trial.
Figure 22: PREMIUM Trial Consort Diagram

As shown in Figure 22 above, in PREMIUM, all patients randomized (gammaCore, n=165; sham, n=167) represent the ITT population. Of these patients, 278 (gammaCore, n=138; sham, n=140) complied with the trial requirement to self-administer no fewer than two-thirds of the specified treatments per month during the randomized period. This population represents an mITT. Demographic and baseline characteristics were generally well balanced between the gammaCore and sham cohorts.
For the ITT and mITT populations, the baseline average number of migraine days per month was similar between the two cohorts (gammaCore, 7.94 and 8.06, respectively; sham, 7.80 and 7.78, respectively). The primary endpoint was not met for the ITT population (gammaCore, -2.26; sham, -1.80; p=0.15; linear regression). However, as shown in Figure 23 below, statistical significance was achieved in reduction of migraine days per month, the primary endpoint metric, for the mITT population (gammaCore, -2.27 migraine days; sham, -1.53 migraine days; p=0.04; linear regression).
118
Table of Contents
Figure 23: Primary Endpoint Analysis of the ITT and mITT Populations for the PREMIUM Trial

As shown in Figures 24 and 25 below, with respect to key secondary and exploratory endpoints, statistical significance was achieved across several measurements in the mITT population. As shown in Figure 24 below, the average percentage reduction in migraine days per month among the mITT population was greater for the gammaCore cohort compared with sham (gammaCore, 26.7%; sham, 16.8%; p<0.05). As shown in Figure 25 below, the reduction in the average number of headache days per month among the mITT population was greater for the gammaCore cohort compared with sham (gammaCore, -2.85; sham, 1.99; p=0.05). The mean reduction in days on which medication was required was statistically significant greater in the gammaCore cohort as compared with sham among the mITT population (gammaCore, -1.94; sham, -1.14; p<0.04). While not reaching statistical significance, the proportion of patients experiencing at least a 50% reduction in migraine days per month demonstrated a trend toward significance consistent with the previously reported endpoints (gammaCore, 31.6%; sham, 22.1%; p<0.08).
Figures 24 and 25: Additional Secondary and Exploratory Endpoint Analysis for the PREMIUM Trial
|
|
|


119
Table of Contents
In our PREMIUM trial, no SAEs were attributed to gammaCore. Of all randomized patients, 25.8% (88/341; gammaCore, 31/169; sham, 57/172) had ³ to 1 ADE during the trial. As shown in Table 9 below, the most commonly occurring ADEs were application site irritation, all of which were non-serious, transient, and tended to be self-limiting in nature. The PREMIUM trial demonstrated that our gammaCore therapy for acute migraine treatment has a highly favorable tolerability profile.
Table 9: Most Commonly Reported ADEs from the PREMIUM Trial

Additional Headache Opportunities
Migraine in Adolescents. Peak migraine penetrance occurs during adolescence and parents may be hesitant to place children on medication. Our clinician advisors have indicated their belief that our gammaCore therapy would be particularly well received in this population given its tolerability profile. We are currently partnered with opinion leaders from academic medical centers and other tertiary headache centers to develop a clinical trial that we expect to initiate in the second half of 2018 to support a label expansion for gammaCore to include patients as young as 12 years of age.
Post-Traumatic Headache. Unlike migraine and CH, which are primary headaches, Post-Traumatic Headaches, or PTH, are classified as secondary headaches because they have a clear causation associated with head trauma. Research has shown that head trauma activates immune cells in the central nervous system. This activation can lead to a disruption in neurotransmitter expression, hyperexcitation, and to the production of CGRP.
VNS, including gammaCore therapy, has been shown to be effective in reducing this immune cell activation. Our clinical and scientific advisors have indicated their belief that our gammaCore therapy has the potential to offer therapeutic benefit for this patient population. We are currently developing a clinical trial that we expect to initiate in the second half of 2018 to support a label expansion for gammaCore to include PTH.
Our Pipeline
Rheumatology
The Anti-inflammatory Mechanisms of VNS
The systemic anti-inflammatory effects of VNS are believed to result from the activation of sympathetic fibers in the splenic nerve, through a connection at the celiac ganglion. These sympathetic fibers release norepinephrine into the spleen in close proximity to a specialized group of immune cells that release acetylcholine, or ACh. This release of ACh activates a receptor, the alpha 7 nicotinic ACh receptor, or a7nAChR, on cytokine-releasing immune cells called macrophages. Activation of these receptors is believed to function by blocking transcription factors that promote inflammatory cytokine expression. Based on the role of ACh in activating this pathway, which is shown in Figure 26 below, it has been termed the cholinergic anti-inflammatory pathway, or CAP.
120
Table of Contents
Figure 26: The Cholinergic Anti-Inflammatory Pathway

Sjôgren’s Syndrome
Paralleling our market penetration strategy in headache, we have chosen to enter rheumatology inSjôgren’s syndrome, a condition with high unmet need and no currently approved disease modifying treatments. We believe that further expansion into other areas of rheumatology from this base of relevance among clinicians will maximize our ability to penetrate areas like rheumatoid arthritis.
Sjôgren’s syndrome is a chronic inflammatory condition characterized by damage to, and ultimate loss of, moisture-producing glands. The primary clinical consequence of this damage is dry mouth and dry eyes, which can cause significant tooth loss and ocular injury. Related similar symptoms can include dry skin, a chronic cough, and vaginal dryness. Primary Sjôgren’s syndrome, defined as being independent of other rheumatologic conditions, affects approximately 600,000 people in the United States, primarily women. Secondary Sjôgren’s syndrome arises in conjunction with other inflammatory conditions, and increases the number of Sjôgren’s sufferers to approximately four million people in the United States.
It is believed that the disease begins with increased inflammatory cytokine levels of interleukin-1 beta, or IL-1ß. The elevated level of IL-1ß is believed to be the underlying cause of the debilitating fatigue and sleepiness, symptoms that are often the cause of the greatest loss in quality of life among Sjôgren’s patients. This fatigue is a symptom of what is referred to as cytokine-induced sickness behavior.
Sickness behavior is a coordinated set of behavioral changes associated with extended periods of inflammation, including inability to concentrate, lethargy, malaise, fatigue, sleepiness, hyperalgesia, depression, and anxiety. These symptoms are common across many conditions in rheumatology.
An initial open label pilot trial of gammaCore for the treatment of primary Sjôgren’s syndrome was funded by the U.K. Arthritis Foundation, the results of which were recently presented at the 2017 American College of Rheumatology annual meeting. This trial enrolled 20 patients, all of whom provided evaluable data. At the beginning of this trial, enrolled patients provided baseline self-assessments of multiple key symptoms of their condition and blood samples were taken to establish baseline cytokine and other biomarker expression levels. During this first visit, patients were treated with gammaCore and additional blood samples were taken 90 minutes after this initial treatment. Patients were instructed to self-administer gammaCore twice daily, each treatment comprising two doses. Patients returned after seven days to provide self-assessments and additional blood samples. Patients continued this treatment protocol through a total of 26 days. On day 28, after a two-day treatment hiatus, patients provided self-assessments of their symptoms and additional blood samples both before, and 90 minutes following a final gammaCore treatment.
121
Table of Contents
As shown in Figure 27 below, cytokine levels of both IL-1ß and TNF-a were significantly reduced from timepoint 1, or baseline, to timepoint 2, 90 minutes following their first treatment with gammaCore. The levels of these cytokines remained at these reduced levels, or lower, at timepoint 3, which was their day seven visit, and timepoints 4 and 5, both of which occurred at their day 28 visit (both before and after their final gammaCore treatments).
Figure 27: Reductions in IL-1ß and TNF-a from baseline through Day 28 in Sjôgren’s syndrome patients using gammaCore therapy.

122
Table of Contents
As shown in Figure 28 below, the clinical results from this open-label pilot trial demonstrated statistical significance for reductions in physical fatigue and sleepiness, and trends toward significance for mental fatigue and abnormal fatigue.
Figure 28: Reductions in key fatigue and sleepiness measurements from baseline through Day 26 in Sjôgren’s syndrome patients using gammaCore therapy.
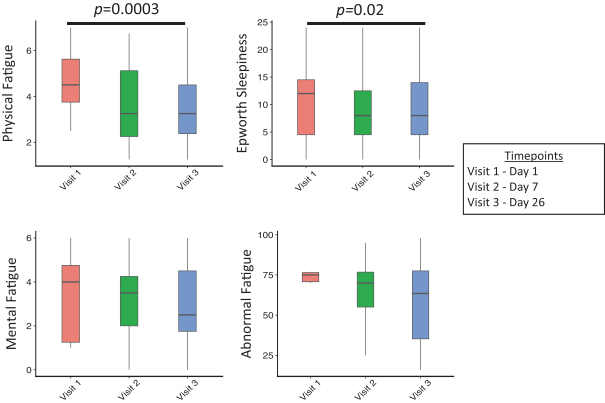
We are currently preparing for a pre-investigational device exemption, or IDE, meeting with the FDA to gain clarity regarding a pivotal trial design that could support an application for a labeling claim for the signs and symptoms of Sjôgren’s syndrome, and confirm that the FDA’s review of such an application would proceed through the de novo pathway.
Rheumatoid Arthritis
Rheumatoid arthritis, or RA, is a chronic autoimmune disorder primarily affecting joints, and in particular the synovial tissue within the joint capsule. The condition is characterized by observable inflammation in the synovial tissue of affected joints, with associated warmth, swelling, pain, and loss of function around the inflammation. Symptoms typically worsen following rest. The most commonly affected areas include smaller joints of the body such as the wrists, hands, and feet, and typically affects the same joints on both sides of the body.
Uncontrolled RA is associated with significant morbidity and increased mortality. The current standard of care involves treating patients early and aggressively to prevent, or significantly retard the progression of joint damage. This is important, as progression of joint damage is directly correlated with debility, disability and loss of function. Approximately 2.4 million patients, predominantly women, suffer from RA in the United States. Current treatments for RA have been shown to possess a disease modifying
123
Table of Contents
effect, in addition to being effective at controlling signs and symptoms. Some agents used in the treatment of RA, most notably the biologics have shown effectiveness in the treatment of psoriatic arthritis and ankylosing spondylitis.
Inflammatory cytokines have long been identified in the pathogenesis of RA. Medications that inhibit immune activity, either broadly, like corticosteroids, or biologic agents, specifically targeting individual cytokines, have been key treatment options for RA patients. Typically, patients with RA initiate treatment with methotrexate, or MTX, which is sufficient to arrest the disease progression and provide relief of the disabling symptoms in approximately 25% of the affected population. Despite being generically available, the average cost of chronic MTX treatment in the United States still averages greater than $200 per month.
Incomplete response to MTX requires additional therapy, typically in the form of a biologic treatment, the most common of which are antibodies or antibody-like proteins that bind to TNF-a. By targeting TNF-a, these treatments alter the normal functioning of the immune system, and as such carry significant risks related to opportunistic infections and several forms of cancers. Approximately 40% of patients with RA are successfully treated with this class of medications, but at an average cost of $30,000 per year. Estimates suggest that of the more than $30 billion of annual global sales of these medications, sales for RA and related conditions of ankylosing spondylitis and psoriatic arthritis exceed $15 billion.
Those patients who are inadequately managed by MTX and/or anti-TNF-a agents, typically advance to other biologic agents that attempt to either block the circulating levels of other target inflammatory cytokines, or block the intracellular pathways that promote the production of inflammatory cytokines. The latter includes the Janus kinase inhibitors, such as Xeljanz, which have an annual cost currently ranging from $40,000 to over $60,000.
Initial clinical evidence for the use of VNS in RA was published in 2016 reporting on an open label pilot trial of implanted VNS among a group of 17 RA patients who had failed standard of care therapy (7 MTX incomplete responders and 10 who had failed at least two biologic agents). As shown in Figure 29 below, the results of this trial demonstrated clinical improvement in disease activity score, or DAS28, over a six-week period of about 2.5 points in MTX incomplete responders and about 1.5 points in biologic failures greater than 1.5 points. Patients had their VNS therapy deactivated for a two-week period following the initial six-week treatment period, during which time DAS28 scores rapidly returned to prior activity levels. This trend reversed and trended towards improvement when VNS therapy was re-initiated.
Figure 29: Mean change in DAS scores reported following implantation of and activation of VNS devices.

124
Table of Contents
We are currently preparing for a pre-IDE meeting with the FDA to confer with its reviewers regarding a multi-center, randomized, double blind, sham-controlled trial of gammaCore therapy for the treatment of RA and to confirm that the FDA’s review of such an application would proceed through the de novo pathway for a signs and symptoms labeling claim.
Manufacturing
We are the FDA-registered manufacturer of our gammaCore products. We rely upon third-party suppliers, located both within and outside the United States, for substantially all of the component parts of gammaCore, including injection molded housings, printed circuit board assemblies, batteries, electrodes and conductive gel.
At our facility in Basking Ridge, NJ, we inspect the component parts following receipt to ensure they meet their design specifications. This quality inspection involves physical measurements and electrical performance testing. After successful completion of this inspection, our proprietary software is loaded into the microcontroller located on the printed circuit board. The battery and electrodes are connected to the printed circuit board, which is then placed in a plastic housing. The gammaCore is then configured to deliver the number of days of therapy to be prescribed, and a final test is performed on the unit to ensure it meets our performance specifications. The unit is then packaged, along with appropriate labeling, instructions for use and conductive gel, and shipped into our distribution network.
We currently have sufficient capacity to meet anticipated demand for our therapy for the foreseeable future. As demand rises, we may choose to maximize operating efficiencies by transferring manufacturing to one or more company-approved contract manufacturers. We are currently evaluating potential third-party manufacturers; however, we do not anticipate such a transfer will occur prior to 2019.
In order to protect against the risk of supply chain disruption, we are qualifying alternative vendors and suppliers to ensure timely access to components necessary for the manufacture and assembly of our gammaCore products. We will also retain the expertise and capabilities to fulfill our commercial product needs internally, if necessary. These measures include purchasing a sufficient advanced supply of key components to reasonably assure that no component shortages will interrupt our ability to manufacture and deliver our products to patients on a timely basis.
The generation of our proprietary signal does not require custom electronic components. Therefore, we believe long-term supply agreements with our suppliers are not necessary as all the components used in our products are either high-volume, non-custom commodity components, or are readily available from multiple vendors. The majority of these components have multiple sources, and the few with single-sources have been purchased with sufficient reserves to permit continued production of our product should simple design modifications be required.
Coverage and Reimbursement
Commercial payors in the United States typically make coverage and reimbursement decisions with respect to new therapies based on three key factors: the strength of the therapy’s clinical data; initial patient demand; and the absolute and relative cost of the therapy. Our payor engagement strategy was initiated eighteen months prior to market entry, with pipeline presentations across the largest two-dozen commercial payors in the United States. We engaged with payors directly and through experienced consultants specializing in securing coverage and reimbursement. Many of these payors have indicated that we should advocate for reimbursement of our product as a pharmacy benefit. This pathway may allow patients to obtain our therapy through payment of a co-payment rather than being personally responsible for the costs of our product until meeting an annual deductible. The pathway may also permit payors to manage utilization of gammaCore through different tiers of coverage requiring varying co-pay amounts, prior authorizations, and requirements that patients fail less expensive treatments
125
Table of Contents
before gaining access to more expensive therapies. While some commercial payors may provide coverage under their pharmacy benefit plans, other payors, including governmental and private insurers, may not be willing or authorized to provide coverage for our therapy under pharmacy plans that more commonly cover prescription drug products. These payors may require us to seek coverage for gammaCore as a medical supply or item of durable medical equipment, which could result in the application of different pricing, reimbursement, and patient cost-sharing policies to our products.
Our strategy has been to gain early access for the narrowly defined market of CH where patients have only one other FDA-approved commercially available acute treatment option. To address the key factors used to make coverage and reimbursement decisions, we provide payors published data from our multiple clinical trials. Our commercial product registry is designed to generate patient demand in the form of prescriptions submitted to the payors. In concert with this commercial registry, we have established a comprehensive publication program to highlight evidence of the high cost of CH patients and to support the use of gammaCore as a cost-effective treatment option. To demonstrate this, we hired a pharmacy benefit management company that reviewed data from four of its regional health plans, totaling 2.5 million members. This review revealed that pharmacy costs for CH patients were double that of patients in a matched group of non-CH sufferers, and were 2.3 times more likely to be prescribed an opioid. However, many third-party payors do not currently cover our products because they have determined gammaCore and other non-invasive VNS treatments to be experimental or investigational.
In addition, the U.S. government, state legislatures and foreign governments have continued implementing cost-containment programs, including price controls and restrictions on coverage and reimbursement. Adoption of price controls and cost-containment measures, and adoption of more restrictive policies in jurisdictions with existing controls and measures, could limit our net sales and results. Decreases in third-party reimbursement for our products or decisions by third-party payors to not cover our products could reduce physician utilization of our products and have a material adverse effect on our sales, results of operations and financial condition.
Commercialization
Our commercial strategy will initially focus on the following priorities:
| • | Drive advocacy of gammaCore as a leading headache therapy. Our strategy is to establish gammaCore as a preferred treatment option, initially in eCH and expanding into migraine. We are developing advocacy for gammaCore among key opinion leaders through our clinical program and initial product registry. We currently have in excess of 250 clinicians trained on gammaCore use. Of these, 50 are key opinion leaders who will lead a series of training and educational programs to advocate for gammaCore use among their colleagues. Through the second quarter of 2018, we have scheduled 50 peer-to-peer educational programs, which will be led by these key opinion leaders. An additional 150 such programs are scheduled for the third and fourth quarters of 2018. |
| • | Drive reimbursement of our therapy. Through our product registry we are generating prescriptions and patient claims to prompt commercial payors to initiate clinical review and subsequent reimbursement policies for gammaCore. We have engaged over 50 national and regional commercial insurance payors in the United States with the goal of obtaining reimbursement coverage as a pharmacy benefit. Reimbursement policies for gammaCore as a pharmacy benefit are currently in place for 2.1 million commercial lives. Our access negotiations have entered the active clinical review stage with more than a dozen additional insurance plans covering approximately 120 million additional commercial lives. |
| • | Build a leading commercial presence. We have partnered with an established specialty pharmacy network to provide physician and patient support to quickly onboard patients and manage payor interactions. This support includes adjudication of all gammaCore |
126
Table of Contents
| prescriptions, payor claims for reimbursement, and patient support and training. Our sales force targets high-prescribing neurology practices and headache centers in the United States. Currently, our sales force consists of four regional business directors and 13 territory business managers. In addition, four medical science liaisons provide medical affairs support. We plan to hire an additional 19 territory business managers, who will ultimately cover 6,000 high-prescribers of headache medications. |
Our Proprietary gammaCore Ecosystem. We continue to focus on fostering advocacy among key opinion leaders and securing reimbursement policies with payors by leveraging the high unmet need in CH, setting the stage for our expansion into migraine. Consistent with this strategy, we have structured our distribution around a pharma-like model, forming an essential piece of our proprietary stakeholder-connecting ecosystem. This ecosystem engages patients, physicians, insurance providers, and our specialty pharmacy in a network that offers these stakeholders:
| • | Physician ease of use. Physicians can enter prescriptions through a web-based interface engaging our trained care specialists to register new patients; |
| • | Rapid prescription insurance adjudication. These care specialists work with our specialty pharmacy partner to accelerate the insurance adjudication process, contacting the physician and/or the patient if additional information is required; |
| • | Concierge patient engagement and personalized training. The specialty pharmacy contacts the patient to obtain the co-pay, ships gammaCore directly to the patient’s home, reviews the contents of the shipment with the patient on delivery, trains the patient on gammaCore use, and follows up within 48 hours to answer any additional questions the patient may have; and |
| • | Ongoing patient support. Care specialists follow up with patients every month to answer any questions, remind them of refills, and support compliance with the therapy. |
A key feature of the highly connected ecosystem we have constructed is our HIPAA-compliant, cloud-based data warehouse. The web portal feature of this network enables unprecedented engagement with patients through which we can provide training and educational material, and offer interactive diaries that provide us real-time feedback. This interactive experience will be expanded to engage with patients through their smart phones, informing them of key information such as the distance they are from their gammaCore and the time to their next dose or refill. In the future, we intend to incorporate additional features that may allow the smartphone to assist patients with identification and/or prediction of their risk factors and triggers. The portal is designed to promote patient engagement and the ability for the ecosystem to improve treatment outcomes.
The logistics of gammaCore distribution are significantly more efficient than that of traditional pharmaceutical therapies. Pharmaceutical therapies are typically distributed through a multi-tiered supply chain involving wholesalers, warehoused supply centers, and individual pharmacy branches, all of which separate the patient from the manufacturer.
By connecting our proprietary data warehouse directly to our specialty pharmacy partner, gammaCore’s distribution eliminates several tiers of the traditional supply chain. Each gammaCore can be refilled electronically through the delivery of unique digital authorization codes, which are maintained in this cloud-based warehouse. We provide these codes to our specialty pharmacy partner by permitting its access to the database, and to the patient through RFID cards programmed by the pharmacists we have trained. More specifically, following adjudication of the prescription and securing payment or payor authorization, this trained pharmacist is granted access to our cloud-based system and programs an RFID card, in real-time, using a tablet computer that we provide. This digital warehouse has the capability to provide refill authorization codes directly from the warehouse to the patient through
127
Table of Contents
Bluetooth technology, further increasing the ease and efficiency of prescription refills by eliminating the need for RFID cards.
An important limitation of the traditional pharmaceutical distribution model is that manufacturers can only track prescriptions through the purchase of data from a third party, which is typically several months old, making real-time responsiveness impossible. Our system captures real-time information regarding the patient, therapy usage, and refill status. All sales and marketing data are completely current, and available at a maximally granular level, enabling real-time decision-making.
Competition
While we believe that our proprietary gammaCore therapy provides us with competitive advantages, we face potential competition from many different sources, including pharmaceutical, biotechnology and other healthcare companies. In addition, academic institutions, governmental agencies and public and private research institutions are actively conducting research in overlapping fields of interest. Our gammaCore therapy will compete with existing therapies and therapies that may become available in the future.
We believe the key competitive factors affecting the success of our therapy are its safety, efficacy, convenience, price, the availability of generic drugs and the availability of coverage and reimbursement from government and other third-party payors.
Many of the companies we are competing with now, or with which we may compete in the future, have significantly greater financial resources and expertise in research and development, manufacturing, preclinical testing, conducting clinical trials, obtaining regulatory approvals and marketing approved drugs than we do. Smaller or early-stage companies may also prove to be significant competitors, particularly through collaborative arrangements with large and established companies. These competitors also compete with us in recruiting and retaining qualified scientific and management personnel and establishing clinical trial sites and patient registration for clinical trials, as well as in acquiring technologies complementary to, or necessary for, our programs.
In primary headache, we face competition from companies that develop and/or sell the following types of treatments:
Treatments for Cluster Headache
The most frequently used acute treatments for CH attacks are subcutaneous sumatriptan and inhaled oxygen. Alternative treatments include intranasal triptans and intravenous DHE. Only subcutaneous sumatriptan and intravenous DHE are approved in the United States for the acute treatment of CH. There are currently no FDA-approved commercially available medications for the prevention of CH. Medications that are used off-label include verapamil, lithium, and valproate.
Treatments for Migraine
The most frequently prescribed therapy for the acute treatment of migraine are oral or nasal triptans. Additional prescribed products include prescription strength NSAIDs. Small molecule CGRP receptor agonists are currently in development by Allergan and Biohaven Pharmaceuticals for the acute treatment of migraines. Certain classes of anti-epileptic medicine and beta-blocker medications have been approved by the FDA for the prevention of migraine. There is currently only one therapy approved for the prevention of chronic migraine, BOTOX. There are currently four antibodies to CGRP and its receptor in development by Alder, Teva, Eli Lilly and Amgen for the prevention of migraine. There are a number of medical devices that have been marketed for the treatment of migraine, including Cefaly and the Spring TMS device.
128
Table of Contents
Intellectual Property
We actively seek to protect the intellectual property and proprietary technology that we believe is important to our business, which includes seeking and maintaining patents covering our technology and products, proprietary processes and any other inventions that are commercially or strategically important to the development of our business. We also rely upon trademarks to build and maintain the integrity of our brand, and we seek to protect the confidentiality of trade secrets that may be important to the development of our business. For more information, please see “Risk Factors—Risks Related to Intellectual Property.”
Patents and Patent Applications
As of February 1, 2018, we held more than 140 patents and patent applications, including more than 70 issued U.S. patents, more than 25 U.S. patent applications, and more than 40 international patents and applications. All of our current issued patents are projected to expire between 2026 and 2033.
More specifically, our current therapy embodies a number of critical proprietary innovations, including a patented high-frequency burst signal that is capable of passing comfortably through the capacitance of the skin. In addition, our therapy utilizes a patented low pass filtration that substantially eliminates high frequency harmonics that would otherwise activate pain receptors in the skin. The combined result is a mild sensation that activates the target fibers in the cervical vagus nerve. While physically possible to administer electricity through the skin of the neck that will activate the same vagal fibers without these innovations, the intensity of pain receptor activation makes it virtually impossible to do so without causing unacceptably high pain levels.
Additionally, we have claims covering the methods of treating various headache conditions using our innovative therapy. We also have claims covering our innovative distribution capabilities, including the remote network-enabled communication for delivery of neuromodulation therapy for a broad range of medical conditions.
The term of individual patents depends on the legal term for patents in the countries in which they are granted. In most countries, including the United States, the patent term is generally 20 years from the earliest claimed filing date of a non-provisional patent application in the applicable country. We cannot assure you that patents will be issued from any of our pending applications or that, if patents are issued, they will be of sufficient scope or strength to provide meaningful protection for our technology. Notwithstanding the scope of the patent protection available to us, a competitor could develop treatment methods or devices that are not covered by our patents. Furthermore, numerous U.S. and foreign issued patents and patent applications owned by third parties exist in the fields in which we are developing products. Because patent applications can take many years to issue, there may be applications unknown to us, which applications may later result in issued patents that our existing or future products or proprietary technologies may be alleged to infringe.
There has been substantial litigation regarding patent and other intellectual property rights in the medical device industry. In the future, we may need to engage in litigation to enforce our issued patents, to protect our trade secrets or know-how, to defend against claims of infringement of the rights of others or to determine the scope and validity of the proprietary rights of others. Litigation could be costly and could divert our attention from other functions and responsibilities. Adverse determinations in litigation could subject us to significant liabilities to third parties, could require us to seek licenses from third parties and could prevent us from manufacturing, selling or using our gammaCore products, any of which could severely harm our business.
Copyrights, Trademarks and Trade Secrets
The software programs associated with gammaCore and our proprietary ecosystem are protected by U.S. copyright law.
129
Table of Contents
As of February 1, 2018, our trademark portfolio contained six U.S. trademark registrations, including electroCore®, gammaCore® and gammaCore Sapphire®, four pending U.S. trademark applications and one registered European trademark, electroCore®.
We also rely upon trade secrets, know-how and continuing technological innovation, and may pursue licensing opportunities in the future, to develop and maintain our competitive position. We seek to protect our proprietary rights through a variety of methods, including confidentiality agreements and proprietary information agreements with suppliers, employees, consultants and others who may have access to proprietary information, under which they are bound to assign to us inventions made during the term of their employment or term of service.
Government Regulation
United States
Our products and operations are subject to extensive and rigorous regulation by the U.S. Food and Drug Administration, or FDA, under the Federal Food, Drug, and Cosmetic Act, or FFDCA, and its implementing regulations, guidance documentation, and standards. Our gammaCore products are regulated by the FDA as medical devices. The FDA regulates the design, development, research, testing, manufacturing, safety, labeling, storage, recordkeeping, promotion, distribution, sale and advertising of medical devices in the United States to ensure that medical products distributed domestically are safe and effective for their intended uses. The FDA also regulates the export of medical devices manufactured in the United States to international markets. Any violations of these laws and regulations could result in a material adverse effect on our business, financial condition and results of operations. In addition, if there is a change in law, regulation or judicial interpretation, we may be required to change our business practices, which could have a material adverse effect on our business, financial condition and results of operations.
Under the FFDCA, medical devices are classified into one of three classes—Class I, Class II or Class III—depending on the degree of risk associated with each medical device and the extent of control needed to ensure safety and effectiveness.
Class I devices are those for which safety and effectiveness can be assured by adherence to FDA’s “general controls” for medical devices, which include compliance with the applicable portions of the FDA’s Quality System Regulation, or QSR, facility registration and product listing, reporting of adverse medical events, and appropriate, truthful and non-misleading labeling, advertising, and promotional materials. Some Class I devices also require premarket clearance by the FDA through the 510(k) premarket notification process described below.
Class II devices are subject to FDA’s general controls, and any other “special controls” deemed necessary by FDA to ensure the safety and effectiveness of the device, such as performance standards, product-specific guidance documents, special labeling requirements, patient registries or post-market surveillance. Premarket review and clearance by the FDA for Class II devices is accomplished through the 510(k) premarket notification procedure, though certain Class II devices are exempt from this premarket review process. When a 510(k) is required, the manufacturer must submit to the FDA a premarket notification submission demonstrating that the device is “substantially equivalent” to a legally marketed device, which in some cases may require submission of clinical data. Unless a specific exemption applies, 510(k) premarket notification submissions are subject to user fees. If the FDA determines that the device, or its intended use, is not substantially equivalent to a legally marketed device, the FDA will place the device, or the particular use of the device, into Class III, and the device sponsor must then fulfill much more rigorous premarketing requirements.
Class III devices, consisting of devices deemed by the FDA to pose the greatest risk, such as life-sustaining, life-supporting or implantable devices, or devices deemed not substantially equivalent to a
130
Table of Contents
predicate device. The safety and effectiveness of Class III devices cannot be assured solely by general or special controls. Submission and FDA approval of a premarket approval, or PMA, application is required before marketing of a Class III device can proceed. As with 510(k) submissions, unless subject to an exemption, PMA submissions are subject to user fees. The PMA process is much more demanding than the 510(k) premarket notification process. A PMA application, which is intended to demonstrate that the device is safe and effective, must be supported by extensive data, typically including data from preclinical studies and human clinical trials.
510(k) Clearance
To obtain 510(k) clearance for a medical device, an applicant must submit to the FDA a premarket notification submission demonstrating that the proposed device is “substantially equivalent” to a legally marketed device, known as a “predicate device.” A legally marketed predicate device may include a device that was legally marketed prior to May 28, 1976 for which a PMA is not required (known as a “pre-amendments device” based on the date of enactment of the Medical Device Amendments of 1976), a device that has been reclassified from Class III to Class II or Class I, or a device that was found substantially equivalent through the 510(k) process. A device is substantially equivalent if, with respect to the predicate device, it has the same intended use and has either (i) the same technological characteristics, or (ii) different technological characteristics, but the information provided in the 510(k) submission demonstrates that the device does not raise new questions of safety and effectiveness and is at least as safe and effective as the predicate device. A showing of substantial equivalence sometimes, but not always, requires clinical data.
Before the FDA will accept a 510(k) submission for substantive review, the FDA will first assess whether the submission satisfies a minimum threshold of acceptability. If the FDA determines that the 510(k) submission is incomplete, the FDA will issue a “Refuse to Accept” letter which generally outlines the information the FDA believes is necessary to permit a substantive review and to reach a determination regarding substantial equivalence. An applicant must submit the requested information before the FDA will proceed with additional review of the submission. Once the 510(k) submission is accepted for review, by regulation, the FDA has 90 days to review and issue a determination. As a practical matter, clearance often takes longer. The FDA may require additional information, including clinical data, to make a determination regarding substantial equivalence.
If the FDA agrees that the device is substantially equivalent to a predicate device currently on the market, it will grant 510(k) clearance to commercially market the device. If the FDA determines that the device is “not substantially equivalent” to a previously cleared device, the device is automatically designated as a Class III device. The device sponsor must then fulfill more rigorous PMA requirements, or can request a risk-based classification determination for the device in accordance with the “de novo” process, which is a route to market for novel medical devices that are low to moderate risk and are not substantially equivalent to a predicate device.
After a device receives 510(k) marketing clearance, any modification that could significantly affect its safety or effectiveness, or that would constitute a major change or modification in its intended use, will require a new 510(k) marketing clearance or, depending on the modification, PMA approval. The determination as to whether or not a modification could significantly affect the device’s safety or effectiveness is initially left to the manufacturer using available FDA guidance. Many minor modifications today are accomplished by a “letter to file” in which the manufacture documents the rationale for the change and why a new 510(k) is not required. However, the FDA may review such letters to file to evaluate the regulatory status of the modified product at any time and may require the manufacturer to cease marketing and recall the modified device until 510(k) clearance or PMA approval is obtained. The manufacturer may also be subject to significant regulatory fines or penalties.
131
Table of Contents
PMA Approval
A PMA must be submitted to the FDA for any device that is classified in Class III or otherwise cannot be cleared through the 510(k) process (although the FDA has discretion to continue to allow certain pre-amendment Class III devices to use the 510(k) process). PMA applications must be supported by, among other things, valid scientific evidence demonstrating the safety and effectiveness of the device, which typically requires extensive data, including technical, preclinical, clinical and manufacturing data. The PMA must also contain a full description of the device and its components, a full description of the methods, facilities, and controls used for manufacturing, and proposed labeling. Following receipt of a PMA application, once the FDA determines that the application is sufficiently complete to permit a substantive review, the FDA will formally accept the application for review. The FDA, by statute and by regulation, has 180-days to review an “accepted” PMA application, although the review of an application more often occurs over a significantly longer period of time, and can take up to several years. During the review period, the FDA will typically request additional information or clarification of the information already provided. Also, an advisory panel of experts from outside the FDA may be convened to review and evaluate the application and provide recommendations to the FDA as to the approvability of the device. The FDA may or may not accept the panel’s recommendation. In addition, the FDA will generally conduct a pre-approval inspection of the manufacturing facility or facilities to ensure compliance with the QSR.
If the FDA evaluations of both the PMA application and the manufacturing facilities are favorable, the FDA will either issue an approval letter or an approvable letter, which usually contains a number of conditions that must be met in order to secure final approval of the PMA. If the FDA’s evaluation of the PMA or manufacturing facilities is not favorable, the FDA will deny approval of the PMA or issue a not approvable letter. A not approvable letter will outline the deficiencies in the application and, where practical, will identify what is necessary to make the PMA approvable. The FDA may also determine that additional clinical trials are necessary, in which case the PMA approval may be delayed for several months or years while the trials are conducted. Once granted, PMA approval may be withdrawn by the FDA if compliance with post-approval requirements, conditions of approval or other regulatory standards is not maintained or problems are identified following initial marketing.
In approving a PMA the FDA may also require some form of post-market surveillance when necessary to protect the public health or to provide additional safety and effectiveness data for the device. In such cases, the manufacturer might be required to follow certain patient groups for a number of years and makes periodic reports to the FDA on the clinical status of those patients.
New PMAs or PMA supplements are required for modifications that affect the safety or effectiveness of a PMA-approved device, including, for example, certain types of modifications to the device’s indication for use, manufacturing process, labeling and design. PMA supplements often require submission of the same type of information as a PMA, except that the supplement is limited to information needed to support any changes from the device covered by the original PMA and may not require as extensive clinical data or the convening of an advisory panel.
De Novo Classification
Medical device types that the FDA has not previously classified as Class I, II or III are automatically classified into Class III regardless of the level of risk they pose. The Food and Drug Administration Modernization Act of 1997 established a new route to market for low to moderate risk medical devices that are automatically placed into Class III due to the absence of a predicate device, called the “Request for Evaluation of Automatic Class III Designation,” or the de novo classification procedure. This procedure allows a manufacturer whose novel device is automatically classified into Class III to request down-classification of its medical device into Class I or Class II on the basis that the device presents low or moderate risk, rather than requiring the submission and approval of a PMA application. Prior to the
132
Table of Contents
enactment of the Food and Drug Administration Safety and Innovation Act of 2012, or the FDASIA, a medical device could only be eligible for de novo classification if the manufacturer first submitted a 510(k) premarket notification and received a determination from the FDA that the device was not substantially equivalent. FDASIA streamlined the de novo classification pathway by permitting manufacturers to request de novo classification directly without first submitting a 510(k) premarket notification to the FDA and receiving a not substantially equivalent determination. Under FDASIA, the FDA is required to classify the device within 120 days following receipt of the de novo application. If the manufacturer seeks reclassification into Class II, the manufacturer must include a draft proposal for special controls that are necessary to provide a reasonable assurance of the safety and effectiveness of the medical device. In addition, the FDA may reject the reclassification petition if it identifies a legally marketed predicate device that would be appropriate for a 510(k) or determines that the device is not low to moderate risk or that general controls would be inadequate to control the risks and special controls cannot be developed.
In March 2014 we filed a pre-submission package with the FDA requesting a meeting to discuss the viability of using the de novo pathway to gain authorization to commercialize our gammaCore product for an initial indication in CH. In June 2014, FDA met with us and confirmed that the de novo pathway would be appropriate for our submission. In October 2014 we filed our initial de novo application with FDA. As is customary for many applications for commercial approval (Class II or Class III), FDA in a letter to us in May 2015 denied our initial application stating that our initial filing did not yet support a de novo clearance based on the information in the initial filing. In June 2015 we participated in an in person meeting with FDA representatives to discuss the issues raised by the FDA in its May 2015 denial letter. In October 2015, based on our June 2015 meeting with FDA, we resubmitted our de novo application with two proposed indications: (i) acute treatment of eCH; and (ii) prophylactic treatment of cCH. In February 2016, we received a letter from FDA indicating that our de novo application, with some further requested re-analysis, included sufficient data to support de novo classification and clearance of gammaCore for at least one indication. We performed and submitted to the FDA the requested re-analysis in March 2016 and, following additional correspondence and meetings with FDA, in April 2017, FDA approved our de novo classification request and cleared our gammaCore therapy in the United States for the acute treatment of pain associated with eCH in adults.
Based on this approval, of our de novo classification request, gammaCore has been down classified to Class II under a new Class II device regulatory category for non-invasive cervical vagus nerve stimulators for the treatment of headache. The establishment of this category created a 510(k) regulatory pathway for the potential expansion of the gammaCore label to include acute treatment and/or prevention of pain associated with migraine and cCH, as well as acute treatment and/or prevention of other primary and secondary headaches. In January 2018, the FDA cleared gammaCore for acute treatment of pain associated with migraine headaches in adult patients, and we have conducted several additional clinical studies with a view to supporting additional label expansion.
Additionally, we anticipate utilizing the de novo classification process to obtain marketing authorization for our product candidates under development outside the headache field.
Clinical Studies
When FDA clearance or approval of a Class I, Class II or Class III device requires human clinical trials, and if the device presents a “significant risk” to human health, the device sponsor is required to file an IDE application with the FDA and obtain IDE approval prior to commencing the human clinical trial. If the device is considered a “non-significant risk,” IDE submission to FDA is not required. Instead, only approval from the Institutional Review Board, or IRB, overseeing the investigation at each clinical trial site is required. Human clinical studies are generally required in connection with approval of Class III devices and may be required for Class I and II devices. The FDA or the IRB at each institution at which a
133
Table of Contents
clinical trial is being performed may suspend a clinical trial at any time for various reasons, including a belief that the subjects are being exposed to an unacceptable health risk. Even if a trial is completed, the results of clinical testing may not adequately demonstrate the safety and efficacy of the device or may otherwise not be sufficient to obtain FDA clearance or approval to market the product in the United States.
Continuing Regulation
After a device is placed on the market, numerous regulatory requirements apply. These include:
| • | Product listing and establishment registration, which helps facilitate FDA inspections and other regulatory action; |
| • | QSR, which requires manufacturers, including third-party manufacturers, to follow stringent design, testing, control, documentation and other quality assurance procedures during all aspects of the design and manufacturing process; |
| • | labeling regulations and FDA prohibitions against the promotion of products for uncleared or unapproved “off-label” uses; |
| • | clearance of product modifications that could significantly affect safety or efficacy or that would constitute a major change in intended use of one of our cleared devices; |
| • | approval of product modifications that affect the safety or effectiveness of one of our approved devices; |
| • | medical device reporting regulations, which require that manufacturers comply with FDA requirements to report if their device may have caused or contributed to a death or serious injury, or has malfunctioned in a way that would likely cause or contribute to a death or serious injury if the malfunction of the device or a similar device were to recur; |
| • | post-approval restrictions or conditions, including post-approval study commitments; |
| • | post-market surveillance regulations, which apply when necessary to protect the public health or to provide additional safety and effectiveness data for the device; |
| • | the FDA’s recall authority, whereby it can ask, or under certain conditions order, device manufacturers to recall from the market a product that is in violation of governing laws and regulations; |
| • | regulations pertaining to voluntary recalls; and |
| • | notices of corrections or removals. |
Advertising and promotion of medical devices, in addition to being regulated by the FDA, are also regulated by the Federal Trade Commission and by state regulatory and enforcement authorities. Recently, promotional activities for FDA-regulated products of other companies have been the subject of enforcement action brought under healthcare reimbursement laws and consumer protection statutes. In addition, under the federal Lanham Act and similar state laws, competitors and others can initiate litigation relating to advertising claims. If the FDA determines that our promotional materials or training constitutes promotion of an unapproved or uncleared use, it could request that we modify our training or promotional materials or subject us to regulatory or enforcement actions. It is also possible that other federal, state or foreign enforcement authorities might take action if they consider our promotional or training materials to constitute promotion of an unapproved or uncleared use, which could result in significant fines or penalties under other statutory authorities, such as laws prohibiting false claims for reimbursement. In that event, our reputation could be damaged and adoption of the products would be impaired.
134
Table of Contents
Furthermore, our products could be subject to voluntary recall if we or the FDA determine, for any reason, that our products pose a risk of injury or are otherwise defective. Moreover, the FDA can order a mandatory recall if there is a reasonable probability that our gammaCore therapy would cause serious adverse health consequences or death.
The FDA has broad post-market and regulatory enforcement powers. We are subject to unannounced inspections by the FDA to determine our compliance with the QSR and other regulations, and these inspections may include the manufacturing facilities of some of our subcontractors. Failure by us or by our suppliers to comply with applicable regulatory requirements can result in enforcement action by the FDA or other regulatory authorities, which may result in sanctions including, but not limited to:
| • | untitled letters, warning letters, fines, injunctions, consent decrees and civil penalties; |
| • | unanticipated expenditures to address or defend such actions |
| • | customer notifications for repair, replacement, refunds; |
| • | recall, detention or seizure of our products; |
| • | operating restrictions or partial suspension or total shutdown of production; |
| • | refusing or delaying our requests for 510(k) clearance or PMA approval of new products or modified products; |
| • | operating restrictions; |
| • | withdrawing 510(k) clearances or PMA approvals that have already been granted; |
| • | refusal to grant export approval for our products; or |
| • | criminal prosecution. |
To date, our facility has not been inspected by the FDA.
International
Our international sales are subject to regulatory requirements in the countries in which our products are sold. The regulatory review process varies from country to country and may in some cases require the submission of clinical data.
We have received CE Mark approval in Europe for our gammaCore therapy to treat, among other indications, primary headaches, including migraines, and asthma.
In the EEA, gammaCore must comply with the Essential Requirements laid down in Annex I to Directive 93/42/EEC on the approximation of the laws of the Member States relating to medical devices or the EU Medical Devices Directive. Compliance with these requirements is a prerequisite to be able to affix the CE mark to gammaCore, without which they cannot be marketed or sold in the EEA. To demonstrate compliance with the Essential Requirements and obtain the right to affix the CE Mark medical devices manufacturers must undergo a conformity assessment procedure, which varies according to the type of medical device and its classification. Except for low risk medical devices (Class I with no measuring function and which are not sterile), where the manufacturer can issue an EC Declaration of Conformity based on a self-assessment of the conformity of its products with the Essential Requirements, a conformity assessment procedure requires the intervention of a Notified Body, which is an organization designated by a competent authority of an EEA country to conduct conformity assessments. Depending on the relevant conformity assessment procedure, the Notified Body would audit and examine the Technical File and the quality system for the manufacture, design and final inspection of the medical devices. The Notified Body issues a CE Certificate of Conformity following successful completion of a
135
Table of Contents
conformity assessment procedure conducted in relation to the medical device and its manufacturer and their conformity with the Essential Requirements. This Certificate entitles the manufacturer to affix the CE mark to its medical devices after having prepared and signed a related EC Declaration of Conformity.
As a general rule, demonstration of conformity of medical devices and their manufacturers with the Essential Requirements must be based, among other things, on the evaluation of clinical data supporting the safety and performance of the products during normal conditions of use. Specifically, a manufacturer must demonstrate that the device achieves its intended performance during normal conditions of use and that the known and foreseeable risks, and any adverse events, are minimized and acceptable when weighed against the benefits of its intended performance, and that any claims made about the performance and safety of the device (e.g., product labeling and instructions for use) are supported by suitable evidence. This assessment must be based on clinical data, which can be obtained from (1) clinical studies conducted on the devices being assessed, (2) scientific literature from similar devices whose equivalence with the assessed device can be demonstrated or (3) both clinical studies and scientific literature. With respect to Class III devices, the manufacturer must conduct clinical studies to obtain the required clinical data, unless reliance on existing clinical data from equivalent devices can be justified. The conduct of clinical studies in the EEA is governed by detailed regulatory obligations. These may include the requirement of prior authorization by the competent authorities of the country in which the study takes place and the requirement to obtain a positive opinion from a competent Ethics Committee. This process can be expensive and time-consuming.
Moreover, in May 2017, the EU Medical Devices Regulation (Regulation 2017/745) was adopted. The EU Medical Devices Regulation repeals and replaces the EU Medical Devices Directive. Unlike directives, which must be implemented into the national laws of the EEA Member States, the regulations would be directly applicable, i.e., without the need for adoption of EEA Member State laws implementing them, in all EEA member States and are intended to eliminate current differences in the regulation of medical devices among EEA member States. The EU Medical Devices Regulation, among other things, is intended to establish a uniform, transparent, predictable and sustainable regulatory framework across the EEA for medical devices and ensure a high level of safety and health while supporting innovation. The EU Medical Devices Regulation will however only become applicable three years after publication (in May 2020). Once applicable, the new regulations will among other things:
| • | strengthen the rules on placing devices on the market and reinforce surveillance once they are available; |
| • | establish explicit provisions on manufacturers’ responsibilities for the follow-up of the quality, performance and safety of devices placed on the market; |
| • | improve the traceability of medical devices throughout the supply chain to the end-user or patient through a unique identification number; |
| • | set up a central database to provide patients, healthcare professionals and the public with comprehensive information on products available in the EU; |
| • | strengthened rules for the assessment of certain high-risk devices which may have to undergo an additional check by experts before they are placed on the market. |
Other Regulations
We are also subject to healthcare fraud and abuse regulation in the jurisdictions in which we will conduct our business. These laws include, without limitation, applicable anti-kickback, false claims, physician sunshine and patient privacy and security laws and regulations.
Anti-Kickback Statute: The federal Anti-Kickback Statute prohibits, among other things, persons or entities from knowingly and willfully soliciting, offering, receiving or paying any remuneration, directly
136
Table of Contents
or indirectly, overtly or covertly, in cash or in kind, in exchange for or to induce either the referral of an individual for, or the purchase, lease, order or recommendation of, any good, facility, item or service for which payment may be made, in whole or in part, under federal healthcare programs such as Medicare and Medicaid. The federal Anti-Kickback Statute is broad and prohibits many arrangements and practices that are lawful in businesses outside of the healthcare industry. The term “remuneration” includes kickbacks, bribes, or rebates and also has been broadly interpreted to include anything of value, including for example, gifts, discounts, the furnishing of supplies or equipment, credit arrangements, payments of cash, waivers of payments, ownership interests, relieving a referral source of a financial or administrative burden and providing anything at less than its fair market value. In addition, longstanding OIG guidance makes clear that the opportunity for a referring physician to earn a profit, including through an investment in an entity for which he or she generates business, could constitute illegal remuneration under the Anti-Kickback Statute. The Anti-Kickback Statute is violated if even one purpose of the remuneration is to induce such referrals.
There are a number of narrow statutory exceptions and regulatory safe harbors protecting certain defined business arrangements from prosecution under the federal Anti-Kickback Statute. These statutory exceptions and safe harbors set forth provisions that, if all their applicable requirements are met, will assure healthcare providers and other parties that they may not be prosecuted under the federal Anti-Kickback Statute. The failure of a transaction or arrangement to fit precisely within one or more applicable statutory exceptions or safe harbors does not necessarily mean that it is illegal or that prosecution will be pursued. However, conduct and business arrangements that do not fully satisfy all requirements of an applicable safe harbor may result in increased scrutiny by government enforcement authorities and will be evaluated on a case-by-case basis based on a cumulative review of all of its facts and circumstances. Further, a person or entity does not need to have actual knowledge of the statute or specific intent to violate it in order to have committed a violation. In addition, the government may assert that a claim including items or services resulting from a violation of the federal Anti-Kickback Statute constitutes a false or fraudulent claim for purposes of the federal civil False Claims Act which is discussed below. Penalties for violations of the Anti-Kickback Statute include, but are not limited to, civil monetary penalties up to $74,792 for each violation, plus up to three times the remuneration involved, criminal fines of up to $100,000 and imprisonment of up to 10 years, disgorgement, individual imprisonment, possible exclusion from Medicare, Medicaid and other federal healthcare programs, and the curtailment or restructuring of operations.
In the event that third-party payors require us to be a DME supplier or we sell our products directly to providers who are DME suppliers that submit claims to such payors, we may be subject to the federal Stark physician self-referral law, which prohibits a physician from making a referral for certain designated health services covered by the Medicare program, including DME, if the physician or an immediate family member has a financial relationship with the entity providing the designated health services, and prohibits that entity from billing or presenting a claim for the designated health services furnished pursuant to the prohibited referral, unless an exception applies. Sanctions for violating the Stark Law include denial of payment, civil monetary penalties of up to $24,253 per claim submitted and exclusion from the federal health care programs. Failure to refund amounts received as a result of a prohibited referral on a timely basis may constitute a false or fraudulent claim and may result in civil penalties and additional penalties under the FCA. The statute also provides for a penalty of up to $161,692 for a circumvention scheme. Various states also have corollary laws to the Stark Law, including laws that require physicians to disclose any financial interest they may have with a healthcare provider to their patients when referring patients to that provider. Both the scope and exceptions for such laws vary from state to state.
Federal Civil False Claims Act: The federal civil False Claims Act prohibits, among other things, persons or entities from knowingly presenting or causing to be presented a false or fraudulent claim to, or the knowing use of false statements to obtain payment from or approval by, the federal government.
137
Table of Contents
In addition, private individuals have the ability to bring actions under the civil False Claims Act in the name of the government alleging false and fraudulent claims presented to or paid by the government (or other violations of the statutes) and to share in any amounts paid by the entity to the government in fines or settlement. Such suits, known as qui tam actions, have increased significantly in the healthcare industry in recent years. Manufacturers can be held liable under these laws if they are deemed to “cause” the submission of false or fraudulent claims by, for example, providing inaccurate billing or coding information to customers or promoting a product off-label. Penalties for a federal civil False Claims Act violation include three times the actual damages sustained by the government, plus mandatory civil penalties of between from $11,181 to $22,363 for each false claim, plus treble damages, the potential for exclusion from participation in federal healthcare programs. The majority of states also have statutes or regulations similar to the federal Anti-Kickback and False Claims Act, which apply to items and services reimbursed under Medicaid and other state programs, or, in several states, apply regardless of the payor.
Civil Monetary Penalties. The Civil Monetary Penalty Act of 1981 imposes penalties against any person or entity that, among other things, is determined to have presented or caused to be presented a claim to a federal healthcare program that the person knows or should know is for an item or service that was not provided as claimed or is false or fraudulent, or offering or transferring remuneration to a federal healthcare beneficiary that a person knows or should know is likely to influence the beneficiary’s decision to order or receive items or services reimbursable by the government from a particular provider or supplier.
Federal Healthcare Fraud Laws. Other federal healthcare fraud-related laws also provide criminal liability for violations. The Criminal Healthcare Fraud statute (18 U.S.C. § 1347) prohibits knowingly and willfully executing a scheme to defraud any healthcare benefit program, including private third-party payors. Federal criminal law at 18 U.S.C. § 1001, among other sections, prohibits knowingly and willfully falsifying, concealing, or covering up a material fact or making any materially false, fictitious, or fraudulent statement in connection with the delivery of or payment for healthcare benefits, items, or services.
Health Insurance Portability and Accountability Act of 1996: The federal Health Insurance Portability and Accountability Act, or HIPAA, created several new federal crimes, including healthcare fraud and false statements relating to healthcare matters. The healthcare fraud statute prohibits knowingly and willfully executing, or attempting to execute, a scheme to defraud any healthcare benefit program, including private third-party payors. The false statements statute prohibits knowingly and willfully falsifying, concealing or covering up a material fact or making any materially false, fictitious or fraudulent statement in connection with the delivery of or payment for healthcare benefits, items or services. Similar to the federal Anti-Kickback Statute, a person or entity does not need to have actual knowledge of the statute or specific intent to violate it in order to have committed a violation.
In addition, HIPAA and its implementing regulations established uniform standards for certain covered entities, which are healthcare providers, health plans and healthcare clearinghouses, as well as their business associates and subcontractors, governing the conduct of specified electronic healthcare transactions and protecting the security and privacy of protected health information. HIPAA, as amended by the Health Information Technology for Economic and Clinical Health Act, or HITECH created four new tiers of civil monetary penalties and gave state attorneys general new authority to file civil actions for damages or injunctions in federal courts to enforce the federal HIPAA laws and seek attorneys’ fees and costs associated with pursuing federal civil actions. Additionally, certain states have adopted comparable privacy and security laws and regulations, some of which may be more stringent than HIPAA and HITECH.
The Federal Physician Payments Sunshine Act: The federal Physician Payments Sunshine Act requires certain manufacturers of drugs, devices, biologics and medical supplies for which payment is available
138
Table of Contents
under Medicare, Medicaid or the Children’s Health Insurance Program, with certain exceptions, to report annually to the Centers for Medicare & Medicaid Services, or CMS, information related to “payments or other transfers of value” made to physicians (defined to include doctors, dentists, optometrists, podiatrists and chiropractors) and teaching hospitals, and to report annually to CMS certain ownership and investment interests held by physicians and their immediate family members. Failure to submit required information may result in civil monetary penalties of $11,052 per failure up to an aggregate of $165,786 per year (or up to an aggregate of $1.105 million per year for “knowing failures”), for all payments, transfers of value or ownership or investment interests that are not timely, accurately, and completely reported in an annual submission, and may result in liability under other federal laws or regulations. Certain states also require device manufacturers to report information related to payments and other transfers of value to physicians and other healthcare providers or marketing expenditures, require pharmaceutical companies to comply with the industry’s voluntary compliance guidelines and the applicable compliance guidance promulgated by the U.S. federal government, or otherwise restrict payments that may be made to healthcare providers and other potential referral sources.
EU Data Protection Legislation: We are subject to laws and regulations in non-U.S. countries covering data privacy and the protection of health-related and other personal information. EU member states and other jurisdictions have adopted data protection laws and regulations, which impose significant compliance obligations. For example, the EU Data Protection Directive, as implemented into national laws by the EU member states, imposes strict obligations and restrictions on the ability to collect, analyze and transfer personal data, including health data from clinical trials and adverse event reporting. Failing to comply with these laws could lead to government enforcement actions and significant penalties against us, and adversely impact our operating results. The EU General Data Protection Regulation, or GDPR, will become applicable on May 25, 2018 and will replace the EU Data Protection Directive. Unlike the Directive (which needed to be implemented by national laws), the GDPR is directly applicable in each EU Member State, resulting in a more uniform application of data privacy laws across the EU. The GDPR imposes stricter requirements and onerous accountability obligations on companies that process personal data, especially if they process sensitive personal data (such as data concerning health). Fines for non-compliance with the GDPR will be significant – up to € 20 million or 4% of global turnover, whichever is higher.
The Foreign Corrupt Practices Act: The Foreign Corrupt Practices Act, or FCPA, prohibits any U.S. individual or business from paying, offering, or authorizing payment or offering of anything of value, directly or indirectly, to any foreign official, political party or candidate for the purpose of influencing any act or decision of the foreign entity in order to assist the individual or business in obtaining or retaining business. The FCPA also obligates companies whose securities are listed in the United States to comply with accounting provisions requiring the company to maintain books and records that accurately and fairly reflect all transactions of the corporation, including international subsidiaries, and to devise and maintain an adequate system of internal accounting controls for international operations.
Healthcare Reform
The United States and some foreign jurisdictions are considering or have enacted a number of legislative and regulatory proposals to change the healthcare system in ways that could affect our ability to sell our products profitably. Among policy makers and payors in the United States and elsewhere, there is significant interest in promoting changes in healthcare systems with the stated goals of containing healthcare costs, improving quality or expanding access. Current and future legislative proposals to further reform healthcare or reduce healthcare costs may limit coverage of or lower reimbursement for our products. The cost containment measures that payors and providers are instituting and the effect of any healthcare reform initiative implemented in the future could impact our revenue from the sale of our products.
139
Table of Contents
The implementation of the Affordable Care Act in the United States, for example, has changed healthcare financing and delivery by both governmental and private insurers substantially, and affected medical device manufacturers significantly. The Affordable Care Act imposed, among other things, a new federal excise tax on the sale of certain medical devices, which, through a series of legislative amendments, was suspended for 2016 through 2019, and which, absent further legislative action, will be reinstated on medical device sales starting January 1, 2020; provided incentives to programs that increase the federal government’s comparative effectiveness research, and implemented payment system reforms including a national pilot program on payment bundling to encourage hospitals, physicians and other providers to improve the coordination, quality and efficiency of certain healthcare services through bundled payment models. Additionally, the Affordable Care Act has expanded eligibility criteria for Medicaid programs and created a new Patient-Centered Outcomes Research Institute to oversee, identify priorities in, and conduct comparative clinical effectiveness research, along with funding for such research. We do not yet know the full impact that the Affordable Care Act will have on our business. There have been judicial and Congressional challenges to certain aspects of the Affordable Care Act, and we expect additional challenges and amendments in the future. Moreover, the Trump Administration and the U.S. Congress may take further action regarding the Affordable Care Act, including, but not limited to, repeal or replacement. Most recently, the Tax Cuts and Jobs Acts was enacted, which, among other things, removes penalties for not complying with the individual mandate to carry health insurance.
In addition, other legislative changes have been proposed and adopted since the Affordable Care Act was enacted. For example, the Budget Control Act of 2011, among other things, included reductions to Medicare payments to providers of 2% per fiscal year, which went into effect on April 1, 2013 and, due to subsequent legislative amendments to the statute, will remain in effect through 2025 unless additional Congressional action is taken. Additionally, the American Taxpayer Relief Act of 2012, among other things, reduced Medicare payments to several providers, including hospitals, and increased the statute of limitations period for the government to recover overpayments to providers from three to five years.
We expect additional state and federal healthcare reform measures to be adopted in the future, any of which could limit the amounts that federal and state governments will pay for healthcare products and services, which could result in reduced demand for our products or additional pricing pressure.
Employees
As of December 31, 2017, we employed 48 fulltime employees. Substantially all of our employees are located in Basking Ridge, New Jersey. None of our employees are represented by a labor union or covered by a collective bargaining agreement. We consider our relationship with our employees to be good.
Facilities
Our principal offices occupy approximately 25,000 square feet of leased office space in Basking Ridge, New Jersey, pursuant to a lease agreement that expires in April 30, 2022. We believe that our current facilities are suitable and adequate to meet our current needs. We may in the future add new facilities or expand existing facilities as we add employees, and we believe that suitable additional or substitute space will be available as needed to accommodate any such expansion of our operations.
Legal Proceedings
We are not subject to any material legal proceedings.
Glossary
“a7nAChR” refers to a receptor, specifically the alpha 7 nicotinic ACh receptor, that resides on the surface of many cell types, including macrophages and microglia, the dominant immune cell of the brain.
140
Table of Contents
Activation of this receptor by neurotransmitters, including acetylcholine, has been shown to cause a change in the inflammation state mediated by these cells, which has led to this immune modulatory pathway being referred to as “the cholinergic anti-inflammatory pathway”, or “CAP”.
“ACh” means acetylcholine, which is a neurotransmitter released by certain neurons in the brain and by the vagus nerve. ACh is also released by a class of immune cells in response to certain stimuli.
“CAP” means the cholinergic anti-inflammatory pathway, which is an autonomic reflex that inhibits the release of pro-inflammatory proteins called cytokines involving signaling in the vagus nerve, the release of acetylcholine and the activation of alpha 7 nicotinic ACh receptors.
“CGRP” means calcitonin gene–related peptide, which is a protein produced by, and released by neurons. CGRP activates other neurons that are involved in pain perception. CGRP is also known to be a powerful vasodilator, causing dilation of blood vessels.
“CH” means cluster headache, which is a headache disorder in which patients experience attacks of severe head pain, typically centered around the eye on one side, which occur from once every other day to eight times a day for a period that may last for a week, months or years. The attacks typically last 15 minutes to 180 minutes and the pain is typically associated tearing, eyelid dropping, sweating, congestion and/or runny nose.
“cCH” means chronic CH, which is a classification of CH defined by CH attacks occurring for more than one year without remission, or with remission periods lasting less than three months.
“CSD” means cortical spreading depression, which is a slow moving, self-propagated wave of depolarization of neurons and glial cells that spreads across the brain.
“eCH” means episodic CH, which is a classification of CH defined by CH attacks occurring in periods lasting from seven days to one year, separated by pain-free periods lasting at least three months.
“DAS” means disease activity score, which is an assessment used to measure rheumatoid arthritis (RA) disease activity, to determine whether the signs and symptoms have reduced or stopped, and if treatment needs to be adjusted.
“DHE” means dihydroergotamine, which is a medication indicated for medically refractory migraine headaches. Its therapeutic activity has been attributed to activity against certain serotonin receptors, and has potent vasoconstricting effects on intracranial blood vessels.
“EEG” means electroencephalography, which involves the measurement and recording of electrical activity in the brain.
“functional magnetic resonance imaging” is an imaging technique that allows for, among other things, the measurement of brain activity through the detection of changes in blood oxygenation and flow that occur in response to neuronal activity.
“GABA” means gamma-aminobutyric acid, which is one of the primary inhibitory neurotransmitters in the brain.
“IL-1ß“means interleukin-1 beta, which is a pro-inflammatory cytokine involved in immune responses.
“LC” means locus coeruleus, which is a small region of the brainstem that is the sole source of norepinephrine in the brain.
141
Table of Contents
“magnetoencephalography” is an imaging technique utilizing superconducting coils to measure the tiny magnetic fields generated by nerve activity within the brain from outside the skull.
“MTX” means methotrexate, which is an immunosuppressive medication, originally used in oncology, and now used widely as a first line treatment for rheumatoid arthritis (RA) and related inflammatory disorders.
“nVNS” means noninvasive vagus nerve stimulation, which is a therapy employing the modulation of signals carried along certain fibers in the cervical vagus nerve which is achieved by the delivery of electric signals passed through the skin without physically penetrating the body.
“NRM” means the nucleus raphe magnus, which is a structure in the brainstem that is a major component in the endogenous pain inhibitory system and that produces and releases serotonin.
“PAG” means the periaqueductal gray, which is a structure in the brainstem that is a major component in the endogenous pain inhibitory system and that produces and releases the neurotransmitter GABA.
“PTH” means post-traumatic headache, which is a headache condition resembling migraine that results from a traumatic head injury.
“RA” means rheumatoid arthritis, which is a common autoimmune disease characterized by chronic joint inflammation leading to pain, swelling, and ultimately the degeneration of cartilage and bone within the affected joint.
“SN” means the substantia nigra, which is a large midbrain structure that can be divided into two parts, one of which synthesizes and releases a neurotransmitter called dopamine, and the other of which synthesizes and releases the neurotransmitter GABA neurons.
“SPG” means sphenopalatine ganglion, which is a nerve bundle behind the bony structure of the nose that connects to the nerves in and around the eye socket. Activity in the SPG has been associated with CH.
“TCC” means the trigeminal cervical complex, which is a region of the brainstem that serves as a primary center and relay for pain, having inputs known to be associated with the generation and perception of head pain.
“TNF-a” means tumor necrosis factor alpha, which is a pro-inflammatory protein, or cytokine, involved in inflammatory events, and is associated with both the initiation and conclusion of inflammatory processes.
“VNS” means vagus nerve stimulation, which is a therapy involving the triggering of signals within certain fibers of the vagus nerve known to alter biologic function through the promotion of neurotransmitter release.
142
Table of Contents
The following table sets forth the name, age as of February 13, 2018 and position of the individuals who currently serve as executive officers, directors and key employees of Electrocore, LLC, and are expected to continue to serve as the executive officers, directors and key employees of electroCore, Inc. following the corporate conversion and the completion of this offering. The following also includes certain information regarding the individual experience, qualifications, attributes and skills of our executive officers, directors and key employees, as well as brief statements of those aspects of our directors’ backgrounds that led us to conclude that they are qualified to serve as directors.
| Name |
Age | Position(s) | ||||
| Executive officers: |
||||||
| Francis R. Amato |
53 | Chief Executive Officer and Director | ||||
| Joseph P. Errico |
49 | Chief Science and Strategy Officer and Chairman of the Board | ||||
| Peter S. Staats, M.D. |
54 | Chief Medical Officer | ||||
| Glenn S. Vraniak |
55 | Chief Financial Officer | ||||
| Key employees: |
||||||
| Roland D. Duhart |
60 | Chief Commercial Officer | ||||
| Eric J. Liebler |
54 | Senior Vice President, Neurology | ||||
| Steven M. Mendez |
57 | Chief Technical Officer | ||||
| Michael Romaniw |
61 | Vice President, Quality Assurance | ||||
| Bruce J. Simon, Ph.D. |
68 | Vice President, Research | ||||
| Non-employee directors: |
||||||
| Nicholas Colucci |
58 | Director | ||||
| Thomas J. Errico, M.D. |
65 | Director | ||||
| Trevor J. Moody |
52 | Director | ||||
| David M. Rubin, Ph.D. |
52 | Director | ||||
| James L.L. Tullis |
70 | Director | ||||
Executive Officers
Francis R. Amato has served as our Chief Executive Officer since July 2016, and as a member of our board of directors since June 2017. Mr. Amato previously served as our Chief Operating Officer from July 2012 through July 2016. Prior to joining our company, he spent 22 years within the pharmaceutical industry, most recently as Vice President of the Specialty Commercial Operations Group, Global Human Health at Merck & Co. Before joining Merck, Mr. Amato gained extensive commercial experience as Executive Director, Global Business Operations at Schering-Plough, Business Unit Lead, Oncology at Ligand Pharmaceuticals, National Sales Director, Specialty Managed Markets at Pfizer Inc. and National Sales Director, Hospitals at Pharmacia Corporation. Prior to joining the pharmaceutical industry, Mr. Amato was an Infantry Medic in the 82nd Airborne Division of the United States Army. Mr. Amato received his B.A. in Political Science from St. John’s University and his Executive MBA from Pepperdine University’s Graziadio School of Management. Our board of directors believes that Mr. Amato’s extensive senior management experience in the pharmaceutical industry qualifies him for service on our board of directors.
Joseph P. Errico has served as our Chief Science and Strategy Officer since July 2016, and previously served as our Chief Executive Officer from January 2010 to July 2016. Mr. Errico has also served as a member of our board of directors since 2005, when he co-founded our company with Thomas J. Errico and Peter S. Staats, and as chairman of our board of directors since March 2013. Prior to founding our company, Mr. Errico served as the General Manager of the Motion Preservation Unit of Stryker Spine, a Division of Stryker Corporation, from August 2004 through December 2007. Prior to that, Mr. Errico co-founded and served as the Chief Executive Officer and director for Spinecore, Inc., from September
143
Table of Contents
2001 through August 2004, when that company was sold to Stryker Corporation. Mr. Errico received his B.S. in Aeronautical Engineering from the Massachusetts Institute of Technology, his M.S. in Mechanical Engineering and Materials Science from Duke University School of Engineering and his J.D. from Duke University School of Law. Our board of directors believes that Mr. Errico’s extensive senior management experience in innovative healthcare technology companies, and his extensive knowledge and contributions to our company’s intellectual property, products, business, and the science of VNS, qualify him to serve on our board of directors.
Peter S. Staats, M.D. has served as our Chief Medical Officer since May 2017. Dr. Staats also served as a member of our board of directors from 2005, when he co-founded our company with Thomas J. Errico and Joseph P. Errico, until January 2018. Dr. Staats has also served as Chief Medical Officer of National Spine and Pain, LLC, the largest pain practice in the United States, since May 2017. From December 2003 to July 2017, he held the roles of physician and a managing partner of Premier Pain Centers, LLC. Dr. Staats was also the founder of the division of pain medicine in the Department of Anesthesiology and Critical Care Medicine at Johns Hopkins University, where he served as its director for years. He has served the non-profit Positive Outcomes Worldwide as founder and Chief Executive Officer since 2015. Dr. Staats was President of ASIPP, a national Physician Advocacy Organization from 2015 to 2016 and President of the NJ Society of International Pain Physicians, a state Physician Advocacy Organization, from 2013 to 2015. He has served as President of the North American Neuromodulation Society from 2002 to 2003. He has served as Director for the World Institute of Pain since 2015 and is currently chairman of the board of examination for the WIP. Peter received his M.D. from the University of Michigan Medical School and completed his residency and fellowship training at the Johns Hopkins University School of Medicine.
Glenn S. Vraniak has served as our Chief Financial Officer since August 2016. Prior to joining our company, from February 2014 to January 2016, Mr. Vraniak served as Chief Financial Officer at G&W Laboratories, Inc., a specialty pharmaceutical company, where he executed the growth strategy by acquiring two companies and over 35 products. Prior to that, from October 2011 through July 2013, he was President of Aprecia Pharmaceuticals, Inc., a 3D printing technology enabled pharmaceutical company. From 2003 through 2011, Mr. Vraniak was the CFO and Head of Strategic Planning for Prasco Laboratories, a generic pharmaceutical company. From January 2000 to January 2002, he served as Executive VP for GE Capital, and subsequently founded Preceptus, a boutique consulting firm focused on helping small and mid-market companies achieve efficient and scalable growth in the healthcare and technology sectors. Mr. Vraniak received an Electronic Engineering Technology degree and a Managerial MBA in Finance from the Rutgers University Center for Management Development.
Other Key Employees
Roland D. Duhart has served as our Chief Commercial Officer since January 2018, and previously served as our Global Vice President, Sales and Marketing since July 2016. Prior to joining our company, from February 2015 to June 2016, Mr. Duhart held the position of VP, Business Development at Publicis Touchpoint Solutions, a full-service healthcare commercialization company. Previously, from December 2012 to January 2015, he served as Sr. VP, Business Development & Client Services at VMS BioMarketing, a healthcare company. In addition, Mr. Duhart has led sales and marketing teams with increasing scope of responsibility at Schering Plough, Pharmacia-Upjohn, Novartis, and Amylin. Mr. Duhart received his B.S. in Business Administration, Finance from California State University, Northridge.
Eric J. Liebler has served as our Senior Vice President, Neurology since January 2013. Prior to joining our company, Mr. Liebler served from January 2010 to December 2012 as President and member of the board of directors of Nautilus Neurosciences, a neurology-focused pharmaceutical company that he co-founded in 2009. At Nautilus, Mr. Liebler was involved in all facets of the organization and its early success, including initial funding, product commercialization, and sales and marketing. Prior to founding
144
Table of Contents
Nautilus, Mr. Liebler served from September 2007 to December 2008 as Executive Vice President, Corporate Development at Pharmacopeia Inc. Prior to that, he served as Senior Vice President, Strategic Planning and Communication at Questor Pharmaceuticals from August 2006 to September 2007. Mr. Liebler was Managing Partner of Nisola, LLC, a biopharmaceutical consulting firm, from November 2005 to September 2007. He served as Vice President, Business Development at Enzon Pharmaceuticals from December 2002 to November 2005. Previously, Mr. Liebler served as President of Amarin Pharmaceuticals and spent more than 10 years with Elan Corporation and its predecessor Athena Neurosciences, where he served in a number of increasingly senior roles in marketing, investor relations and strategic planning. He also previously served for more than 10 years on the Board of Trustees of the American Academy of Neurology Foundation, now the American Brain Foundation. Mr. Liebler received his B.A. from Tufts University.
Steven M. Mendez has served as our Chief Technical Officer since July 2016, and previously served as Chief Science Officer from 2005 to 2016. Prior to joining our company, from 1998 to 2005, Mr. Mendez was Vice President at EBI, LLC, a subsidiary of Biomet Inc., where he was responsible for electronic, bracing, and softgood products, in addition to overseeing the development of external and implantable electrical/thermal therapy medical devices. Prior to that, Mr. Mendez held engineering positions at Adaptive Instruments Corporation from 1995 to 1998, Walchem Corporation from 1990 to 1994, Wang Laboratories from 1986 to 1989, and United Technologies Corporation from 1983 to 1986. Mr. Mendez received his B.A. in Biology and B.S. in Electrical Engineering from Lehigh University and his M.S. in Electrical Engineering from the Rensselaer Polytechnic Institute.
Michael Romaniw has served as our Vice President, Quality Assurance since January 2011. Prior to joining our company, Mr. Romaniw served as Director of Regulatory Compliance at EBI, LLC, a subsidiary of Biomet Inc. from May 2005 to January 2008, and again from June 2010 to December 2010. Between his periods employment at EBI, Mr. Romaniw held the position of Director of Quality Assurance & Regulatory Compliance at Orthofix Spinal Implants, an affiliate of Blackstone Medical Inc., where he was responsible for product quality control, quality engineering, supplier management, and product complaint handling, as well as the management of field actions and recalls. Prior to that, Mr. Romaniw held various roles relating to manufacturing, design and development, and quality management at companies including Synthes, Sulzer Orthopedics, Kirschner Medical, and 3M Orthopedic Products.
Bruce J. Simon, Ph.D. has served as our Vice President, Research since January 2008. Prior to joining our company, Dr. Simon served as Senior Director of Research at EBI, LLC, a division of Biomet, Inc., from September 1991 to December 2007, where he directed research on the effects of electric and electromagnetic fields on bone, cartilage and soft tissue repair. He has authored or co-authored more than 60 peer-reviewed publications and has 40 issued or pending patents. Dr. Simon obtained a B.S. in Physics from the Massachusetts Institute of Technology and a Ph.D. in Physiology and Biophysics from the University of Iowa. After completing his Ph.D., he spent several years as a Research Assistant Professor at the University of Maryland and then as an Assistant Professor at the University of Texas. His research focused on various aspects of electrophysiology, including excitation-contraction coupling in muscle and biophysical modeling.
Non-employee Directors
Nicholas Colucci has served on our board of directors since August 2017. Since May 2007, Mr. Colucci has been Chief Executive Officer of Publicis Health, a healthcare communications company, and prior thereto, held a variety of account, strategy and leadership roles at Publicis Health, beginning in 1997. Prior to that, Mr. Colucci served as Vice President of Marketing & Sales at EyeSys Technologies (from 1995 to 1997) and as Marketing Director at Hoffman-La Roche (from 1982 to 1995). Mr. Colucci has also previously served on the boards of directors of SDI/Verispan, a healthcare market research company,
145
Table of Contents
and of National Rehab, a wound care distribution company. Mr. Colucci received his B.S. in Neuroscience from the University of Rochester and his M.B.A. from Loyola University Maryland. Our board of directors believes that Mr. Colucci’s background, with more than 30 years of experience across important life sciences and communications industries, qualifies him to serve on our board of directors.
Thomas J. Errico, M.D. has served on our board of directors since September 2005, when he co-founded the company with Joseph P. Errico and Peter S. Staats. Dr. Errico has been a board-certified orthopedic surgeon since 1986, and currently serves as the Chief of Division of Spine Surgery in Orthopedics for NYU Langone Health, a position he has held since 1997. He is also currently a Professor of Orthopedic and Neurologic Surgery in the NYU School of Medicine. In addition, Dr. Errico is a member of the International Society for the Advancement of Spine Surgery, and served as its President from 2010 to 2011. He is also an original member of the North American Spine Society, and served as its President from 2003 to 2004. Dr. Errico has founded multiple companies in the healthcare industry, including Spinecore, Inc. in 2002, where he served as a director until it was sold to Stryker, Inc. in 2004. Dr. Errico was also a founding member of K2M Group Holdings, Inc. in January 2004. Dr. Errico holds a B.S. in Zoology from Rutgers University and an M.D. from Rutgers Medical School, formerly the University of Medicine and Dentistry of New Jersey. Our board of directors believes Dr. Errico is qualified to serve on our board of directors due to his long tenure as a practicing spine-surgeon and his leadership role with a world class academic medical institution, as well as serving as a co-founder, director and investor in a number of successful early stage healthcare companies.
Trevor J. Moody has served on our board of directors since March 2013. Mr. Moody has served since January 2010 as President of TM Strategic Advisors LLC, a management consultancy serving the boards, investors, and senior management of both emerging and established medical technology companies. He also currently serves as Medical Device Partner at MH Carnegie & Co. Pty Ltd (since October 2013), where he makes venture capital investments in medical device companies. From July 2015 to December 2015, Mr. Moody served as interim CEO of a MH Carnegie & Co. portfolio company, Cardiac Dimensions Pty Ltd. From 1999 to 2010, Mr. Moody was at Frazier Healthcare Ventures, a large healthcare-focused venture capital and private equity investment firm. He was a General Partner at Frazier Healthcare Ventures from 2005 to 2010. Prior to that, he was a Senior Consultant at The Wilkerson Group, a leading healthcare strategic consultancy. Mr. Moody currently also serves on the board of trustees of a non-profit called the Center for Infectious Disease Research, and on the boards of several private corporations, including EBR Systems, Inc., Renew Medical Pty Ltd, Serene Medical Pty Ltd, Brain Protection Company Pty Ltd and Simplify Medical Pty Ltd. Mr. Moody received his B.S. in Engineering from the University of Southern Queensland, Australia, and his M.S. in Management from the Massachusetts Institute of Technology (Sloan School). Our board of directors believes that Mr. Moody’s experience, with over 25 years in the development, commercialization and funding of innovative, growth-oriented medical technologies, qualifies him to serve on our board of directors.
David M. Rubin, Ph.D. has served as a member of our board of directors since March 2013. Dr. Rubin is currently a managing director at GHI, where he is responsible for identifying investment opportunities in emerging health care solutions and services, with a particular emphasis on oncology and infectious disease digital health. Prior to joining GHI, Dr. Rubin was portfolio director for Merck & Co.’s MRL Oncology franchise. Dr. Rubin joined Merck in 2007 from Cognia Corporation, a venture-backed research and development software and content products company, where he was the president and chief executive officer. Previously, Dr. Rubin was at The Wilkerson Group/IBM Global Services. Dr. Rubin previously served on the board of VirtualScopics, Inc. (Nasdaq: VSCP) from 2012 through 2014. Dr. Rubin currently serves on the boards of directors of OpGen, Inc., (Nasdaq: OPGN) and Navigating Cancer, Inc. Dr. Rubin was a National Institute of Health and American Cancer Society post-doctoral fellow at Harvard Medical School. Dr. Rubin also received training in post graduate business at Harvard University. Dr. Rubin holds a Ph.D. from Temple University in Molecular Biology and a B.A. from SUNY Binghamton in Biology. Dr. Rubin’s extensive background working with precision medicine and
146
Table of Contents
diagnostic companies, his investing experience, his current executive position with Merck GHI and scientific background make Dr. Rubin a valuable contributor to our board of directors.
James L.L. Tullis has served as a member of our board of directors since July 2014. Mr. Tullis founded Tullis Health Investors, a venture capital firm specializing in investments in the healthcare industry, in 1986, and has served as its Chief Executive Officer since its inception. Prior to that, Mr. Tullis was a Senior Vice President at E.F. Hutton & Co., a stock brokerage firm, and a principal at Morgan Stanley & Co., where he worked with the healthcare investment research and banking teams. Mr. Tullis has served as a member of the board of directors since 2006, and as chairman of the board of directors, since 2017, of Lord Abbett & Co. Mutual Funds, an investment management firm. Since 1998, he has also served as a member of the board of directors of Crane Co., an industrial products manufacturing company. Mr. Tullis also currently serves as a member of the board of directors of several private companies, including LivHOME, Inc., an at-home senior care company, SupplyPro, Inc., an inventory management solutions company, Exagen Diagnostics, Inc., a diagnostics company focused on autoimmune rheumatic diseases, and SafeOp Surgical, Inc., a medical device and technology company. Mr. Tullis holds a B.A. from Stanford University and an M.B.A. from Harvard Business School. Mr. Tullis’ extensive experience serving as a venture capitalist and board member for numerous companies in the health care industry contributed to our board of directors’ conclusion that Mr. Tullis should serve as a director of our company.
Board Composition
Our board of directors currently consists of seven members. The current members of our board of directors have been designated pursuant to the Operating Agreement. The Operating Agreement provides (subject to certain conditions and qualifications specified therein relating to securities ownership and otherwise) that our board is composed of:
| • | one director designated by each of our founding investors, Joseph P. Errico, Dr. Thomas J. Errico, and Kathryn K. Theofilos, two of such seats being filled by Joseph P. Errico and Dr. Thomas J. Errico and one seat being vacant; |
| • | one director designated by Merck GHI, for which Dr. David M. Rubin has been designated; |
| • | one director designated by Core Ventures II, LLC, for which Nicholas Colucci has been designated; |
| • | one director designated by AIH-Electro, LLC, which seat is currently vacant; and |
| • | three other directors designated by the holders of a majority of our outstanding membership units, who have designated Francis R. Amato, Trevor J. Moody and James L.L. Tullis. |
The Operating Agreement also provides that upon the affirmative vote of a majority in interest of each class of our capital stock, voting separately, one additional director may be appointed to our board of directors.
The Operating Agreement will terminate upon the completion of the corporate conversion and, thereafter, our directors will be elected by the vote of our common stockholders. Under our bylaws to be effective upon the completion of the corporate conversion, the number of directors will be determined from time to time by our board of directors.
Each of the current members of our board of directors is expected to serve as a director following the corporate conversion and completion of this offering. At least one new director is expected to be appointed prior to the completion of this offering.
There are no family relationships among any of our directors and executive officers, except that Dr. Thomas J. Errico is the uncle of Joseph P. Errico.
147
Table of Contents
Classified Board of Directors
In accordance with our certificate of incorporation to be effective upon the completion of the corporate conversion, our board of directors will be divided into three classes with staggered, three-year terms. At each annual meeting of stockholders, the successors to directors whose terms then expire will be elected to serve from the time of election and qualification until the third annual meeting following their election. Effective upon the consummation of this offering, we expect that our directors will be divided among the three classes as follows:
| • | the Class I directors will be , and , and their terms will expire at our first annual meeting of stockholders following this offering; |
| • | the Class II directors will be , and , and their terms will expire at our second annual meeting of stockholders following this offering; and |
| • | the Class III directors will be , and , and their terms will expire at our third annual meeting of stockholders following this offering. |
Pursuant to our certificate of incorporation to be effective upon the completion of the corporate conversion, only our board of directors will be able to fill vacancies on our board of directors until the next succeeding annual meeting of stockholders. Any additional directorships resulting from an increase in the number of directors will be distributed among the three classes so that, as nearly as possible, each class will consist of one-third of the directors.
The classification of our board of directors may have the effect of delaying or preventing changes in our control or management. See “Description of Capital Stock—Anti-Takeover Provisions—Our Certificate of Incorporation and Bylaws.”
Director Independence
In connection with this offering, we intend to apply to list our common stock on The Nasdaq Global Select Market, or Nasdaq. Under Nasdaq rules, independent directors must comprise a majority of our board of directors within a specified period of the completion of this offering. In addition, Nasdaq rules require that, subject to specified exceptions, each member of a listed company’s audit, compensation and nominating and governance committees be independent. Under Nasdaq rules, a director will only qualify as an “independent director” if, in the opinion of that company’s board of directors, that person does not have a relationship that would interfere with the exercise of independent judgment in carrying out the responsibilities of a director.
Audit committee members must also satisfy the independence criteria set forth in Rule 10A-3 under the Exchange Act. In order to be considered independent for purposes of Rule 10A-3, a member of an audit committee of a listed company may not, other than in his or her capacity as a member of the audit committee, the board of directors or any other board committee: (i) accept, directly or indirectly, any consulting, advisory or other compensatory fee from the listed company or any of its subsidiaries; or (ii) be an affiliated person of the listed company or any of its subsidiaries.
Prior to the completion of this offering, our board of directors is expected to undertake a review of the independence of each director and consider whether each director has a material relationship with us that could compromise his ability to exercise independent judgment in carrying out his responsibilities. As a result of this review, our board of directors is expected to determine that Messrs. , and , representing of our directors, are “independent directors” as defined under the applicable rules and regulations of the SEC, and the listing requirements and rules of Nasdaq. In making these determinations, our board of directors is expected to review and discuss information provided by the directors and us with regard to each director’s business and personal activities and relationships as
148
Table of Contents
they may relate to us and our management, including the beneficial ownership of our capital stock by each non-employee director and the transactions involving them described in the section entitled “Certain Relationships and Related-Party Transactions.”
Audit Committee
Prior to the closing of this offering, we will establish an audit committee to consist of , and , with serving as chairman. Our board of directors will affirmatively determine that each member of the reconstituted audit committee meets the definition of “independent director” for purposes of the rules and the independence requirements of Rule 10A-3 of the Exchange Act. Our board of directors will also determine which member qualifies as an “audit committee financial expert” under SEC rules and regulations.
Our audit committee will be responsible for, among other matters:
| • | appointing, compensating, retaining, evaluating, terminating and overseeing our independent registered public accounting firm; |
| • | discussing with our independent registered public accounting firm their independence from management; |
| • | reviewing with our independent registered public accounting firm the scope and results of their audit; |
| • | approving all audit and permissible non-audit services to be performed by our independent registered public accounting firm; |
| • | overseeing the financial reporting process and discussing with management and our independent registered public accounting firm the interim and annual financial statements that we file with the Securities and Exchange Commission; |
| • | reviewing and monitoring our accounting principles, accounting policies, financial and accounting controls and compliance with legal and regulatory requirements; |
| • | establishing procedures for the confidential anonymous submission of concerns regarding questionable accounting, internal control or auditing matters; and |
| • | reviewing and approving related person transactions. |
Our board of directors will adopt a new written charter for the audit committee, which will be available on our website.
Compensation Committee
Prior to the closing of this offering, we will reconstitute our compensation committee to consist of , and , with serving as chairman. Our board of directors will affirmatively determine that each member of the reconstituted compensation committee meets the heightened definition of “independent director” for purposes of the Nasdaq rules applicable to members of the compensation committee, and the definition of “non-employee director” for purposes of Section 16 of the Exchange Act.
The compensation committee will be responsible for, among other matters:
| • | establishing and approving, and making recommendations to the board of directors regarding, performance goals and objectives relevant to the compensation of our chief executive officer, evaluating the performance of our chief executive officer in light of those goals and objectives and recommending to the full board of directors for approval, the chief executive officer’s compensation, including incentive-based and equity-based compensation, based on that evaluation; |
149
Table of Contents
| • | setting the compensation of our other executive officers, based in part on recommendations of the chief executive officer; |
| • | reviewing and approving, and making recommendations to the board of directors regarding, employment agreements, severance arrangements and change of control agreements for the chief executive officer and other executive officers, as appropriate; |
| • | exercising administrative authority under our stock plans and employee benefit plans; |
| • | establishing policies and making recommendations to our board of directors regarding director compensation; |
| • | reviewing compensation plans, programs and policies; and |
| • | handling such other matters that are specifically delegated to the compensation committee by the board of directors from time to time. |
Our board of directors will adopt a new written charter for the compensation committee, which will be available on our website.
Nominating and Governance Committee
Prior to the closing of this offering, we will establish a nominating and governance committee to consist of , and , with serving as chairman.
The nominating and governance committee will be responsible for, among other matters:
| • | annually reviewing the list of director selection criteria contained in our corporate governance necessary or appropriate changes thereto; |
| • | identifying, reviewing and evaluating candidates, including candidates submitted by stockholders, for election to our board of directors and recommending to our board of directors (i) nominees to fill vacancies or new positions on our board of directors and (ii) the slate of nominees to stand for election by our stockholders at each annual meeting of stockholders; |
| • | annually recommending to our board of directors (i) the assignment of directors to serve on each committee; (ii) the chairperson of each committee and (iii) the chairperson of our board of directors or lead independent director, as appropriate; |
| • | developing, recommending, overseeing the implementation of and monitoring compliance with, our corporate governance guidelines, and periodically reviewing and recommending any necessary or appropriate changes to our corporate governance guidelines; |
| • | reviewing the adequacy of our certificate of incorporation and bylaws and recommending to our board of directors, as conditions dictate, amendments for consideration by the stockholders; |
| • | reviewing our code of business conduct and ethics and recommending any changes to our board of directors; and |
| • | such other matters as directed by our board of directors. |
Our board of directors will adopt a written charter for the nominating and governance committee, which will be available on our website.
Role of the Board of Directors in Risk Oversight
One of the key functions of our board of directors is informed oversight of our risk management process. The board of directors does not have a standing risk management committee, but rather administers this
150
Table of Contents
oversight function directly through the board of directors as a whole, as well as through various standing committees of our board of directors that address risks inherent in their respective areas of oversight. In particular, our board of directors is responsible for monitoring and assessing strategic risk exposure and our audit committee has the responsibility to consider and discuss our major financial risk exposures and the steps our management has taken to monitor and control these exposures, including guidelines and policies to govern the process by which risk assessment and management is undertaken. The nominating and governance committee will monitor compliance with legal and regulatory requirements and the effectiveness of our corporate governance practices, including whether they are successful in preventing illegal or improper liability-creating conduct. Our nominating and governance committee will also be responsible for overseeing our risk management efforts generally, including the allocation of risk management functions among our board of directors and its committees. Our compensation committee assesses and monitors whether any of our compensation policies and programs has the potential to encourage excessive risk-taking. Our audit committee periodically reviews the general process for the oversight of risk management by our board of directors.
Compensation Committee Interlocks and Insider Participation
As of the closing of the offering, none of the members of our compensation committee will have been at any time during the prior three years one of our officers or employees. As of the closing of the offering, none of our executive officers will serve, or have served in the past fiscal year, as a member of the board of directors or compensation committee of any third party that has one or more executive officers serving on our board of directors or compensation committee.
Code of Business Conduct and Ethics
Prior to the closing of this offering, we will adopt a written code of business conduct and ethics that applies to our directors, officers and employees, including our principal executive officer, principal financial officer, principal accounting officer or controller, or persons performing similar functions. A copy of the code will be posted on our website, which is located at www.electrocore.com. If we make any substantive amendments to, or grant any waivers from, the code of business conduct and ethics for any officer or director, we will disclose the nature of such amendment or waiver on our website or in a current report on Form 8-K. We do not incorporate the information on or accessible through our website into this prospectus, and you should not consider any information on, or that can be accessed through, our website as part of this prospectus.
151
Table of Contents
EXECUTIVE AND DIRECTOR COMPENSATION
Executive Compensation
This section discusses the material components of the executive compensation program offered to our named executive officers and our Chief Financial Officer, whom we refer to as our “NEOs.” For 2017, our NEOs were:
| • | Francis R. Amato, Chief Executive Officer, Director; |
| • | Joseph P. Errico, Chief Science and Strategy Officer, Director; |
| • | Peter S. Staats, M.D., Chief Medical Officer; and |
| • | Glenn S. Vraniak, Chief Financial Officer. |
This discussion may contain forward-looking statements that are based on our current plans, considerations, expectations and determinations regarding future compensation programs. Actual compensation programs that we adopt following the closing of this offering may differ materially from the currently planned programs summarized in this discussion.
We are an “emerging growth company,” within the meaning of the JOBS Act, and have elected to comply with the reduced compensation disclosure requirements available to emerging growth companies under the JOBS Act. See “Prospectus Summary – Implications of Being an Emerging Growth Company.”
2017 Summary Compensation Table
| Name and Principal Position |
Year | Salary ($) | Bonus ($)(1) |
Option Awards ($)(2) |
Non-equity incentive plan compensation($)(3) |
All Other Compensation ($)(4) |
Total ($) | |||||||||||||||||||||
| Francis R. Amato |
2017 | 400,000 | 70,000 | 125,000 | 16,369 | |||||||||||||||||||||||
| Chief Executive Officer, Director |
||||||||||||||||||||||||||||
| Joseph P. Errico |
2017 | 350,000 | 70,000 | — | 16,369 | |||||||||||||||||||||||
| Chief Science & Strategy Officer, Director |
||||||||||||||||||||||||||||
| Peter S. Staats, M.D. |
2017 | 151,667 | (5) | 10,000 | — | 6,820 | ||||||||||||||||||||||
| Chief Medical Officer |
||||||||||||||||||||||||||||
| Glenn S. Vraniak |
2017 | 300,000 | 35,000 | — | 16,369 | |||||||||||||||||||||||
| Chief Financial Officer |
||||||||||||||||||||||||||||
| (1) | Represents discretionary cash bonuses approved by the compensation committee of our board of directors for performance during 2017. |
| (2) | Represents the grant date fair value of Common Units issued as Profits Interests in Electrocore, LLC computed in accordance with FASB ASC 718. See Note 13 to the consolidated financial statements for the fiscal year ended December 31, 2017 included with this prospectus for a description of the assumptions used in valuing our Common Units. These Common Units are intended to constitute profits interests for U.S. federal income tax purposes. Despite the fact that the Common Units that are intended to constitute Profits Interests do not require the payment of an exercise price, we believe they are most similar economically to stock options and are properly classified as “options” under the definition provided in Item 402(a)(6)(i) of Regulation S-K as an instrument with an “option-like feature.” |
| (3) | Represents a contingent cash bonus paid to Mr. Amato following receipt by us of the FDA grant of our de novo application and the closing of our Series B Preferred Unit financing, as discussed below under “—Narrative Disclosure to Summary Compensation Table.” |
| (4) | These amounts consist of payments of health care premiums and contributions to health savings accounts on behalf of the NEO. |
| (5) | Represents a prorated amount of base salary earned by Dr. Staats beginning upon his commencement of employment on May 1, 2017. Pursuant to his employment agreement, Dr. Staats was entitled to an annual base salary of $140,000 for the three calendar months beginning May 1, 2017, and an annual base salary of $280,000 beginning August 1, 2017. |
152
Table of Contents
Narrative Disclosure to Summary Compensation Table
The primary elements of compensation for our NEOs are base salary, annual discretionary bonuses, performance bonuses and equity compensation awards. The NEOs also participate in employee benefit plans and programs that we offer to our other full-time employees on the same basis.
Base Salaries
We pay our NEOs a base salary to compensate them for the satisfactory performance of services rendered to us. The base salary payable to each NEO is intended to provide a fixed component of compensation reflecting the executive’s skill set, experience, role and responsibilities. Base salaries for our NEOs have generally been set at levels deemed necessary to attract and retain individuals with superior talent. No changes to the base salaries of our NEOs occurred for 2017.
Performance Bonuses
We offer our NEOs the opportunity to earn annual discretionary cash bonuses, as determined by our board of directors or the compensation committee annually at their discretion. Actual bonus amounts for our NEOs are determined by our compensation committee after consideration of Mr. Amato and Mr. Errico’s recommendations (except with respect to their individual bonuses).
For 2017, annual bonuses were based on such factors as the board and the compensation committee deemed appropriate, including the FDA grant of our de novo approval, successful completion of our Series B Preferred Unit financing and the individual NEO’s performance as it relates to his area of responsibility. In addition, Mr. Amato received a contractual bonus award required by his employment offer letter.
Equity Compensation
We have granted equity awards to our employees, including our NEOs, as the long-term incentive component of our compensation program. Historically, these awards have consisted of Common Units in Electrocore, LLC that were granted to employees when they commence employment with us. Our Board and Compensation Committee have also from time to time granted additional awards to key employees as they determined appropriate to motivate, retain or reward such employees. These Common Unit grants are intended to qualify as Profits Interests for U.S. federal income tax purposes entitling the holder to participate in our future appreciation from and after the date of grant of the applicable Common Units.
Profits Interests granted to our NEOs are typically subject to time-based vesting conditions and may be subject to accelerated vesting in certain circumstances, including as described below in the sections titled “Unit Forfeiture Agreements” and “—Potential Payments Upon a Change in Control.”
In connection with his elevation to Chief Executive Officer in July 2016 and as additional incentive to retain his services, Mr. Amato was granted 3,500,000 Profits Interests to bring his ownership percentage in the company to 3%, together with certain anti-dilution protection to maintain his ownership at 3% through the final closing of our Series B Preferred Unit financing. Pursuant to such anti-dilution rights, Mr. Amato was granted, in the aggregate, an additional 7,942,573 Profits Interests in 2017 taking into account the final closings of our Series B Preferred Unit financing.
In July 2016, as additional incentive to retain his services, Mr. Errico was granted 1,700,000 Profits Interests, together with certain anti-dilution protection such that 2,400,000 of his Common Units would, as of the final closing of our Series B Preferred Unit financing, represent no less than 2% of our total outstanding capitalization. Pursuant to such anti-dilution rights, Mr. Errico was granted, in the aggregate, an additional 5,321,715 Profits Interests in 2017 taking into account the final closings of our Series B Preferred Unit financing.
153
Table of Contents
In connection with Dr. Staats becoming our Chief Medical Officer on May 1, 2017, Dr. Staats was granted 1,500,000 Profits Interests.
In connection with the hiring of Mr. Vraniak in July 2016 as our Chief Financial Officer, he was granted (i) 225,000 Profits Interests in lieu of his cash salary for the six-month period August 15, 2016 through December 31, 2016, and (ii) 1,700,000 Profits Interests, together with certain anti-dilution protection such that 1,700,000 of his Common Units would, as of the final closing of our Series B Preferred Unit financing, represent no less than 1% of our total outstanding capitalization. Pursuant to such anti-dilution rights, Mr. Vraniak was granted in the aggregate an additional 2,660,858 Profits Interests in 2017 taking into account the final closings of our Series B Preferred Unit financing.
Refer to the Outstanding Equity Awards as of December 31, 2017 table below for a description of the vesting terms that apply to these awards.
In connection with this offering, we intend to adopt the 2018 Plan, to facilitate the grant of cash and equity-based incentives to our directors, employees (including our NEOs) and consultants and to enable us to obtain and retain the services of these individuals, which we believe is essential to our long-term success. For additional information about the 2018 Plan, refer to the section titled “—2018 Incentive Award Plan” below.
Retirement, Health, Welfare and Additional Benefits
Our NEOs are eligible to participate in our employee benefit plans and programs, including medical and dental benefits and flexible spending accounts, to the same extent as our other full-time employees, subject to the terms and eligibility requirements of those plans. We also sponsor a 401(k) defined contribution plan in which our NEOs may participate, subject to limits imposed by the Internal Revenue Code, to the same extent as our other full-time employees. Currently, we do not match any of the contributions made by participants in the 401(k).
Outstanding Equity Awards as of December 31, 2017
The following table sets forth information with respect to outstanding Profits Interests awards for each of our NEOs as of December 31, 2017. For the Profits Interests, the table reflects both vested and unvested units. Profits Interests are subject to time-based vesting and to an additional requirement that a minimum valuation threshold be met before the holder of the Profits Interests is entitled to a distribution in respect of such award.
In connection with the corporate conversion, outstanding Profits Interests of our NEOs will be converted into (i) shares of our common stock, and (ii) provided the NEO is an employee at the time of the conversion, options to purchase our common stock. The number of shares of common stock and the number of options to be issued to each such NEO in respect of his Profits Interests will be determined based upon the appreciation in our value after the date of grant of the applicable Profits Interest through the completion of this offering. The exercise price of these options will be equal to the offering price. Following the corporate conversion, the vesting provisions applicable to the Profits Interests as in effect prior to the corporate conversion will apply, in substantially the same manner, to the shares of common stock and options issued in respect of such Profits Interests in the conversion.
154
Table of Contents
| Option Awards | ||||||||||||||||
| Name |
Number
of Securities Underlying Unexercised Options (#) Exercisable |
Number of Securities Underlying Unexercised Options (#) Unexercisable |
Option Exercise Price ($)(1) |
Option Expiration Date |
||||||||||||
| Francis R. Amato |
700,000 | 0 | $ | 2.75 | — | |||||||||||
| 300,000 | 0 | $ | 0.74 | — | ||||||||||||
| 200,000 | 0 | $ | 0.74 | — | ||||||||||||
| 200,000 | 0 | $ | 0.85 | — | ||||||||||||
| 120,000 | 120,000 | (2) | $ | 0.38 | — | |||||||||||
| 1,312,500 | 2,187,500 | (2) | $ | 0.38 | — | |||||||||||
| 1,846,648 | 3,077,747 | (3) | $ | — | ||||||||||||
| 1,131,817 | 1,886,361 | (3) | $ | — | ||||||||||||
| Joseph P. Errico |
80,000 | 0 | $ | 2.00 | — | |||||||||||
| 1,400,000 | 0 | $ | 0.74 | — | ||||||||||||
| 637,500 | 1,062,500 | (2) | $ | 0.38 | — | |||||||||||
| 1,237,299 | 2,062,164 | (3) | $ | — | ||||||||||||
| 758,345 | 1,263,908 | (3) | $ | — | ||||||||||||
| Peter S. Staats, M.D. |
80,000 | 0 | $ | 2.00 | — | |||||||||||
| 350,000 | 450,000 | (2) | $ | 0.38 | — | |||||||||||
| 0 | 1,500,000 | (2) | $ | 0.17 | — | |||||||||||
| Glenn S. Vraniak |
637,500 | 1,062,500 | (2) | $ | 0.38 | — | ||||||||||
| 225,000 | 0 | $ | 0.38 | — | ||||||||||||
| 618,650 | 1,031,083 | (3) | $ | — | ||||||||||||
| 379,172 | 631,954 | (3) | $ | — | ||||||||||||
| (1) | The Profits Interests do not require the payment of an exercise price. Despite this, we believe they are most similar economically to stock options and are properly classified as “options” under the definition provided in Item 402(a)(6)(i) of Regulation S-K as an instrument with an “option-like feature.” |
| (2) | The awards vest as to 25% of such grant on the one year anniversary of the vesting commencement date and quarterly thereafter in equal installments until fully vested at the fourth anniversary of such award subject to accelerated vesting in certain circumstances as described below under “—Unit Forfeiture Agreements”, or Standard Vesting Schedule. |
| (3) | These awards represent grants in satisfaction of certain anti-dilution protection in favor of certain NEOs. See “—Employment Agreements with Our Named Executive Officers” above. The awards vest in accordance with our Standard Vesting Schedule, but the vesting commencement date for these awards began on the date on which the NEO received a right to anti-dilution protection as described above. |
Effect of the Corporate Conversion and this Offering
Refer to “Management’s Discussion and Analysis of Financial Condition and Results of Operations—Statutory Corporate Conversion” for more information regarding the distribution of our common stock to employees, including our NEOs, in respect of their holdings of our Common Units at the time of the corporate conversion.
Employment Agreements with Our Named Executive Officers
Francis R. Amato
On July 3, 2012, we entered into an employment agreement with Mr. Amato, or the Prior Amato Agreement, providing for base salary, annual target cash bonus opportunity, and standard employee benefit plan participation. In July 2016, we entered into an amended and restated employment agreement, or the Amato Agreement, which superseded and replaced the Prior Amato Agreement in its entirety. Mr. Amato’s base salary currently is $400,000 with an annual target cash bonus opportunity of
155
Table of Contents
up to 17.5% of his annual base salary, payable solely at the discretion of our board of directors. Please see the section above entitled “—2017 Summary Compensation Table—Performance Bonuses” for a further description of the annual bonus awarded to Mr. Amato for 2017. Under the Amato Agreement, Mr. Amato’s employment is terminable at-will and is subject to our standard confidential information and invention assignment provisions and certain non-competition covenants during Mr. Amato’s employment with the Company and, with respect to the non-competition covenant, a period of one year after Mr. Amato’s termination.
Under the Amato Agreement, in the event Mr. Amato’s employment is terminated by us other than for “cause” (as defined below) or as a result of Mr. Amato’s resigning for “good reason” (as defined below), then Mr. Amato will receive (i) a severance payment equal to six months of Mr. Amato’s base salary, payable in equal monthly installments as salary continuation, and (ii) payment or reimbursement by us of COBRA premiums for up to six months.
Under the Amato Agreement, Mr. Amato was granted certain Profits Interests, together with certain anti-dilution protection. See “Equity Compensation” above.
For purposes of the Amato Agreement, “cause” means: (i) Mr. Amato’s gross negligence or willful misconduct in the performance of Mr. Amato’s duties; (ii) the conviction of, or plea of guilty or nolo contendere to, the commission of a felony by Mr. Amato; (iii) the commission of an act of fraud or embezzlement by Mr. Amato against us; or (iv) Mr. Amato’s breach of any material provision of the Amato Agreement.
For purposes of the Amato Agreement, “good reason” means: (i) a material adverse change in Mr. Amato’s position, duties, responsibilities, or status with our company; (ii) a material breach by us of any provision of the Amato Agreement, including without limitation, any reduction in Mr. Amato’s base salary other than in connection with an across the board salary reduction by us for senior management due to material cash flow problems; or (iii) without Mr. Amato’s consent, relocation of his principal business location by us outside of the northern New Jersey/New York metropolitan area.
Joseph P. Errico
On March 28, 2013, we entered into an employment agreement with Mr. Errico, or the Prior Errico Agreement, providing for base salary, performance bonus opportunity, and standard employee benefit plan participation. In July 2016, we entered into an amended and restated employment agreement, or the Errico Agreement, which superseded and replaced the Prior Errico Agreement in its entirety. Mr. Errico’s base salary currently is $350,000 and he is eligible for a performance bonus payable solely at the discretion of our board of directors. Please see the section above entitled “—2017 Summary Compensation Table—Performance Bonuses” for a further description of the annual bonus awarded to Mr. Errico for 2017. Under the Errico Agreement, Mr. Errico’s employment is terminable at-will and is subject to our standard confidential information and invention assignment provisions and certain non-competition covenants during Mr. Errico’s employment with the Company and for the duration that Mr. Errico is receiving severance payments.
Under the Errico Agreement, in the event Mr. Errico’s employment is terminated by us other than for “cause” (as defined below) or as a result of Mr. Errico resigning for “good reason” (as defined below), then Mr. Errico will receive (i) a severance payment equal to 12 months of Mr. Errico’s base salary, payable in equal monthly installments as salary continuation, and (ii) payment or reimbursement by us of COBRA premiums for up to 12 months.
Under the Errico Agreement, Mr. Errico was granted certain Profits Interests, together with certain anti-dilution protection. See “—2017 Summary Compensation Table—Equity Compensation” above.
156
Table of Contents
Peter S. Staats, M.D.
On May 1, 2017, we entered into an employment agreement with Dr. Staats, providing for base salary, annual discretionary bonus opportunity, and standard employee benefit plan participation, or the Staats Agreement. In 2017, Dr. Staats’ base salary was initially $140,000 and increased to $280,000 as of August 1, 2017 and he is eligible for an annual discretionary bonus, as well as reimbursement for expenses associated with continuing medical education credits in connection with maintaining his accreditation as a licensed physician. Please see the section above entitled “—2017 Summary Compensation Table—Performance Bonuses” for a further description of the annual bonus awarded to Dr. Staats’s for 2017. Under the Staats Agreement, Dr. Staats’ employment is terminable at-will and is subject to our standard confidential information and invention assignment provisions and certain non-competition covenants during Dr. Staats’ employment with the Company and for a period of six months after Dr. Staats’ termination.
Glenn S. Vraniak
On July 25, 2016, we entered into an employment agreement with Mr. Vraniak, providing for base salary, annual performance bonus opportunity, and standard employee benefit plan participation, or the Vraniak Agreement. In 2017, Mr. Vraniak’s base salary was $300,000 and he is eligible for an annual performance bonus opportunity, payable solely at the discretion of our board of directors. Please see the section above entitled “—2017 Summary Compensation Table—Performance Bonuses” for a further description of the annual bonus awarded to Mr. Vraniak for 2017. Under the Vraniak Agreement, Mr. Vraniak’s employment is terminable at-will and is subject to our standard confidential information and invention assignment provisions and certain non-competition covenants during Mr. Vraniak’s employment with the Company and, with respect to the non-competition covenant, a period of one year after Mr. Vraniak’s termination.
Under the Vraniak Agreement, in the event Mr. Vraniak’s employment is terminated by us other than for “cause” (as defined below) or as a result of Mr. Vraniak’s resigning for “good reason” (as defined below), then Mr. Vraniak will receive (i) a severance payment equal to six months of Mr. Vraniak’s base salary, payable in equal monthly installments as salary continuation, and (ii) payment or reimbursement by us of COBRA premiums for up to six months.
For purposes of the Errico Agreement and the Vraniak Agreement, “cause” means: (i) the officer’s gross negligence or willful misconduct in the performance of his duties to us; (ii) the conviction of, or plea of guilty or nolo contendere to, the commission of a felony by the officer; (iii) the commission by the officer of an act of fraud or embezzlement against us; or (iv) the officer’s breach of any material provision of the applicable Agreement, subject to prior written notice to him and a reasonable cure period.
For purposes of the Errico Agreement and the Vraniak Agreement, “good reason” means: (i) a material adverse change in the officer’s position, duties, responsibilities, or status with us; (ii) a material breach by us of any provision of his employment agreement, including without limitation, any reduction in his base salary other than in connection with an across the board salary reduction by us for senior management due to material cash flow problems; or (iii) without the officer’s consent, relocation of his principal business location by us outside of the northern New Jersey/New York metropolitan area.
Unit Forfeiture Agreements
In connection with a grant of our Profits Interests, each of our NEOs enters into a standard form of Unit Forfeiture Agreement, which provides for, among other things, acceleration upon a change in control event, as well as upon death or disability. In the event there is a change of control, then one hundred percent of the NEO’s then-unvested Profits Interests will immediately vest, subject to the NEO remaining employed with us until the change in control transaction. Upon an NEO’s death, one hundred percent of
157
Table of Contents
the NEO’s then-unvested Profits Interests will immediately vest and fifty percent of the NEO’s then-unvested Profits Interests will immediately vest upon the NEO’s disability, in both instances subject to the NEO remaining employed with us until such date.
Potential Payments Upon a Change in Control
The unvested Profits Interests held by our NEOs vest in full upon a change in control of our company, subject to the NEO remaining employed with us until the change in control transaction.
2017 Operating Agreement
In November 2017, we amended and restated our Operating Agreement. Our Operating Agreement provides for the grant of Common Units that constitute Profits Interests for income tax purposes to our employees (including officers), non-employee consultants and non-employee directors and those of our affiliates. Under our Operating Agreement, our compensation committee has been delegated the authority to administer the Profits Interests in order to provide a means to attract, retain and motivate our directors, employees and consultants upon whose judgment, initiative and efforts our continued success, growth and development are dependent. In addition to the discretion to grant Profits Interests, the compensation committee sets the vesting terms for awards pursuant to a unit forfeiture agreement. Each Profits Interest includes a minimum valuation threshold that must be achieved before the interest is entitled to receive any distributions under the Operating Agreement. As of December 31, 2017, there were issued and outstanding Profits Interests, of which were vested.
Profits Interests are generally issued pursuant to a Unit Forfeiture Agreement as described above.
Upon the corporate conversion, holders of Profits Interests will be converted into (i) shares of our common stock, and (ii) with respect to holders of Profits Interests who are our employees and consultants at the time of the corporate conversion, options to purchase our common stock. The exercise price of these options will be equal to the offering price. The number of shares of common stock and options to purchase common stock to be issued to each such holder will be determined based upon the appreciation in our value after the date of grant of the applicable Profits Interest through the completion of this offering. Following the corporate conversion, the vesting provisions applicable to the Profits Interests as in effect prior to the corporate conversion will apply, in substantially the same manner, to the shares of common stock and options issued in respect of such Profits Interests.
We anticipate that this equity policy under the current Operating Agreement will be replaced by the 2018 Plan.
2018 Omnibus Incentive Compensation Plan
It is currently anticipated that prior to the completion of this offering, our board of directors and our stockholders will adopt the 2018 Plan.
General
The 2018 Plan will cover the grant of awards to our employees (including officers), non-employee consultants and non-employee directors and those of our affiliates. For purposes of the 2018 Plan , our affiliates include any corporation, partnership, limited liability company, joint venture or other entity, with respect to which we, directly or indirectly, own either (i) stock of a corporation possessing more than fifty percent (50%) of the total combined voting power of all classes of stock entitled to vote, or more than fifty percent (50%) of the total value of all shares of all classes of stock of such corporation, or (ii) an aggregate of more than fifty percent (50%) of the profits interest or capital interest of any non-corporate entity.
We expect that the compensation committee of the board of directors will administer the 2018 Plan. The committee may delegate any or all of its administrative authority to our Chief Executive Officer or to a
158
Table of Contents
management committee except with respect to awards to executive officers who are subject to Section 16 of the Exchange Act. In addition, the full board of directors must serve as the committee with respect to any awards to our non-employee directors.
Up to a maximum of shares of our common stock may be delivered in settlement of awards granted under the 2018 Plan, including upon exercise of incentive stock options. The stock delivered to settle awards made under the 2018 Plan may be authorized and unissued shares or treasury shares, including shares repurchased by us for purposes of the 2018 Plan. If any shares subject to any award granted under the 2018 plan (other than a substitute award as described below) is forfeited or otherwise terminated without delivery of such shares (or if such shares are returned to us due to a forfeiture restriction under such award), the shares subject to such awards will again be available for issuance under the 2018 Plan. However, any shares that are withheld or applied as payment for shares issued upon exercise of an award or for the withholding or payment of taxes due upon exercise of the award will continue to be treated as having been delivered under the 2018 Plan and will not again be available for grant under the 2018 Plan. Upon settlement of any stock appreciation rights, or SARs, the number of shares underlying the portion of the SARs that is exercised will be treated as having been delivered for purposes of determining the maximum number of shares available for grant under the 2018 Plan and shall not again be treated as available for issuance under the 2018 Plan.
If a dividend or other distribution (whether in cash, shares of common stock or other property), recapitalization, forward or reverse stock split, subdivision, consolidation or reduction of capital, reorganization, merger, consolidation, scheme of arrangement, split-up, spin-off or combination involving us or repurchase or exchange of our shares or other securities, or other rights to purchase shares of our securities or other similar transaction or event affects our common stock such that the committee determines that an adjustment is appropriate in order to prevent dilution or enlargement of the benefits (or potential benefits) provided to grantees under the 2018 Plan, the committee will make an equitable change or adjustment as it deems appropriate in the number and kind of securities subject to awards (whether or not then outstanding) and the related exercise price relating to an award in order to prevent dilution or enlargement of the benefits or potential benefits intended to be made available under the 2018 Plan.
Types of Awards
The 2018 Plan permits the granting of any or all of the following types of awards to all grantees:
| • | stock options, including incentive stock options, or ISOs; |
| • | stock appreciation rights, or SARs; |
| • | restricted shares; |
| • | deferred stock and restricted stock units; |
| • | performance units and performance shares; |
| • | dividend equivalents; |
| • | bonus shares; and |
| • | other stock-based awards. |
Generally, awards under the 2018 Plan are granted for no consideration other than prior and future services. Awards granted under the 2018 Plan may, in the discretion of the committee, be granted alone or in addition to, in tandem with or in substitution for, any other award under the 2018 Plan or other plan of ours; provided, however, that if an SAR is granted in tandem with an ISO, the SAR and ISO must have the same grant date and term and the exercise price of the SAR may not be less than the exercise price of the ISO. The material terms of each award will be set forth in a written award agreement between the grantee and us.
159
Table of Contents
Stock Options and SARs
The committee is authorized to grant SARs and stock options (including ISOs except that an ISO may only be granted to an employee of ours or one of our subsidiary corporations). A stock option allows a grantee to purchase a specified number of shares of our common stock at a predetermined price per share (the “exercise price”) during a fixed period measured from the date of grant. An SAR entitles the grantee to receive the excess of the fair market value of a specified number of shares on the date of exercise over a predetermined exercise price per share. The exercise price of an option or an SAR will be determined by the committee and set forth in the award agreement but the exercise price may not be less than the fair market value of a share of common stock on the grant date. The term of each option or SAR is determined by the committee and set forth in the award agreement, except that the term may not exceed 10 years. Options may be exercised by payment of the purchase price through one or more of the following means: payment in cash (including personal check or wire transfer), by delivering shares of our common stock previously owned by the grantee, or with the approval of the committee, by delivery of shares of our common stock acquired upon the exercise of such option or by delivering restricted shares. The committee may also permit a grantee to pay the exercise price of an option through the sale of shares acquired upon exercise of the option through a broker-dealer to whom the grantee has delivered irrevocable instructions to deliver sales proceeds sufficient to pay the purchase price to us.
Restricted Shares
The committee may award restricted shares consisting of shares of our common stock which remain subject to a risk of forfeiture and may not be disposed of by grantees until certain restrictions established by the committee lapse. The vesting conditions may be service-based (i.e., requiring continuous service for a specified period) or performance-based (i.e., requiring achievement of certain specified performance objectives) or both. A grantee receiving restricted shares will have all of the rights of a stockholder, including the right to vote the shares and the right to receive any dividends, except as otherwise provided in the award agreement. Upon termination of the grantee’s affiliation with us during the restriction period (or, if applicable, upon the failure to satisfy the specified performance objectives during the restriction period), the restricted shares will be forfeited as provided in the award agreement.
Restricted Stock Units and Deferred Stock
The committee may also grant restricted stock unit awards and/or deferred stock awards. A deferred stock award is the grant of a right to receive a specified number of shares of our common stock at the end of specified deferral periods or upon the occurrence of a specified event, which satisfies the requirements of Section 409A of the Internal Revenue Code. A restricted stock unit award is the grant of a right to receive a specified number of shares of our common stock upon lapse of a specified forfeiture condition (such as completion of a specified period of service or achievement of certain specified performance objectives). If the service condition and/or specified performance objectives are not satisfied during the restriction period, the award will lapse without the issuance of the shares underlying such award.
Restricted stock units and deferred stock awards carry no voting or other rights associated with stock ownership until the shares underlying the award are delivered in settlement of the award. The award agreement will provide whether grantees may receive dividend equivalents with respect to restricted stock units or deferred stock, and if so, whether such dividend equivalents are distributed when credited or deemed to be reinvested in additional shares of restricted stock units or deferred stock.
Performance Units
The committee may grant performance units, which entitle a grantee to cash or shares conditioned upon the fulfillment of certain performance conditions and other restrictions as specified by the committee and reflected in the award agreement. The initial value of a performance unit will be determined by the
160
Table of Contents
committee at the time of grant. The committee will determine the terms and conditions of such awards, including performance and other restrictions placed on these awards, which will be reflected in the award agreement.
Performance Shares
The committee may grant performance shares, which entitle a grantee to a certain number of shares of common stock, conditioned upon the fulfillment of certain performance conditions and other restrictions as specified by the committee and reflected in the award agreement. The committee will determine the terms and conditions of such awards, including performance and other restrictions placed on these awards, which will be reflected in the award agreement.
Bonus Shares
The committee may grant fully vested shares of our common stock as bonus shares on such terms and conditions as specified in the award agreement.
Dividend Equivalents
The committee is authorized to grant dividend equivalents which provide a grantee the right to receive payment equal to the dividends paid on a specified number of shares of our common stock. Dividend equivalents may be paid directly to grantees or may be deferred for later delivery under the 2018 Plan. If deferred such dividend equivalents may be credited with interest or may be deemed to be invested in shares of our common stock or in other property. No dividend equivalents may be granted in conjunction with any grant of stock options or SARs.
Other Stock-Based Awards
In order to enable us to respond to material developments in the area of taxes and other legislation and regulations and interpretations thereof, and to trends in executive compensation practices, the 2018 Plan authorizes the committee to grant awards that are valued in whole or in part by reference to or otherwise based on our securities. The committee determines the terms and conditions of such awards, including consideration paid for awards granted as share purchase rights and whether awards are paid in shares or cash.
Merger, Consolidation or Similar Corporate Transaction
If there is a merger or consolidation of us with or into another corporation or a sale of substantially all of our stock, or, collectively, a Corporate Transaction, and the outstanding awards are not assumed by surviving company (or its parent company) or replaced with economically equivalent awards granted by the surviving company (or its parent company), the committee will cancel any outstanding awards that are not vested and nonforfeitable as of the consummation of such Corporate Transaction (unless the committee accelerates the vesting of any such awards) and with respect to any vested and nonforfeitable awards, the committee may either (i) allow all grantees to exercise options and SARs within a reasonable period prior to the consummation of the Corporate Transaction and cancel any outstanding options or SARs that remain unexercised upon consummation of the Corporate Transaction, or (ii) cancel any or all of such outstanding awards (including options and SARs) in exchange for a payment (in cash, or in securities or other property) in an amount equal to the amount that the grantee would have received (net of the exercise price with respect to any options or SARs) if the vested awards were settled or distributed or such vested options and SARs were exercised immediately prior to the consummation of the Corporate Transaction. If an exercise price of the option or SAR exceeds the fair market value of our common stock and the option or SAR is not assumed or replaced by the surviving company (or its parent company), such options and SARs will be cancelled without any payment to the grantee.
161
Table of Contents
Amendment to and Termination of the 2018 Plan
The 2018 Plan may be amended, altered, suspended, discontinued or terminated by our board of directors without further stockholder approval, unless such approval of an amendment or alteration is required by law or regulation or under the rules of any stock exchange or automated quotation system on which the common stock is then listed or quoted. Thus, stockholder approval will not necessarily be required for amendments which might increase the cost of the 2018 Plan or broaden eligibility. Stockholder approval will not be deemed to be required under laws or regulations that condition favorable treatment of grantees on such approval, although our board of directors may, in its discretion, seek stockholder approval in any circumstance in which it deems such approval advisable. No ISOs may be awarded after any amendment to the 2018 Plan that either broadens eligibility or increase the number of shares available for delivery in the form of ISOs unless such amendment is approved by our stockholders within 12 months of the date the board of directors approve the adoption of such amendment.
In addition, subject to the terms of the 2018 Plan, no amendment or termination of the 2018 Plan may materially and adversely affect the right of a grantee under any award granted under the 2018 Plan.
Unless earlier terminated by our board of directors, the 2018 Plan will terminate when no shares remain reserved and available for issuance or, if earlier, on , 2028.
Director Compensation
Other than with respect to Mr. Moody as described below, we have historically generally not provided cash retainers to any of our non-employee directors. We have, upon a member joining our Board, granted awards of Profits Interests to our non-employee directors as compensation for their service on our board. We have also, from time to time, granted Profits Interests to certain board members for service on special committees.
2017 Director Compensation Table
The following table provides information regarding the compensation earned during 2017 by our non-executive directors:
| Name |
Fees Earned or Paid in Cash ($) |
Option
Awards ($)(4) |
Total ($) | |||||||||
| Trevor J. Moody |
$ | 20,000 | (1) | $ | 0 | $ | 20,000 | |||||
| Nicholas Colucci |
$ | 0 | $ | $ | ||||||||
| Thomas J. Errico, M.D. |
$ | 0 | $ | 0 | $ | 0 | ||||||
| David M. Rubin, Ph.D. |
$ | 0 | $ | 0 | $ | 0 | ||||||
| James L.L. Tullis |
$ | 0 | $ | 0 | $ | 0 | ||||||
| Kathryn Theofilos |
$ | 0 | $ | 0 | $ | 0 | ||||||
| Peter S. Staats, M.D.(2) |
$ | 0 | $ | 0 | $ | 0 | ||||||
| Reese Terry(3) |
$ | 0 | $ | 0 | $ | 0 | ||||||
| Jeffrey N. Vinik |
$ | 0 | $ | 0 | $ | 0 | ||||||
| (1) | Mr. Moody receives $5,000 per quarter for serving on our board of directors. |
| (2) | Dr. Staats did not receive any compensation for his service as a director in 2017. Dr. Staats’ compensation for his service as our Chief Medical Officer is fully reflected in “—2017 Summary Compensation table” above. Dr. Staats ceased serving as a member of our board of directors in January 2018. |
| (3) | Mr. Terry served on our board of directors until August 2017. |
| (4) | Represents the grant date fair value of Common Units issued as Profits Interests in Electrocore, LLC computed in accordance with FASB ASC 718. See Note 13 to the consolidated financial statements for the fiscal year ended December 31, 2016 included with this prospectus for a description of the assumptions used in valuing our Common Units. These Common Units are intended to constitute profits interests for U.S. federal income tax purposes. Despite the fact that the Common Units that are intended to constitute profits interests do not require the payment of an exercise price, we believe they are most similar economically to stock options and are properly classified as “options” under the definition provided in Item 402(a)(6)(i) of Regulation S-K as an instrument with an “option-like feature.” |
162
Table of Contents
The table below shows the number of vested and unvested Profits Interests, by grant date, held as of December 31, 2017 by each person who served as a non-employee director during the year ended December 31, 2017. The Profits Interests held by Dr. Staats as of December 31, 2017 are reflected in the “Outstanding Awards” table above.
| Grant Date | Total | Profits Interests Vested and Unvested |
||||||||||||||
| Name |
Vested | Unvested | ||||||||||||||
| Nicholas Colucci |
12/1/2017 | 150,000 | 0 | 150,000 | (1) | |||||||||||
| Thomas J. Errico, M.D. |
1/1/2009 | 80,000 | 80,000 | 0 | ||||||||||||
| Trevor J. Moody |
4/1/2013 | 80,000 | 80,000 | 0 | ||||||||||||
| 9/27/2016 | 400,000 | 125,000 | 275,000 | (1) | ||||||||||||
| Reese Terry |
7/5/2014 | 80,000 | 80,000 | 0 | ||||||||||||
| 9/27/2016 | 400,000 | 400,000 | 0 | |||||||||||||
| James L.L. Tullis |
8/1/2014 | 80,000 | 80,000 | 0 | ||||||||||||
| Jeffrey N. Vinik |
— | — | — | — | ||||||||||||
| Kathryn K. Theofilos |
— | — | — | — | ||||||||||||
| David M. Rubin, Ph.D. |
— | — | — | — | ||||||||||||
| (1) | Each award vests 25% at the first anniversary of the award, and thereafter vests quarterly in equal installments until fully vested at the fourth anniversary. Each award is also subject to acceleration upon a change of control event, as well as upon death or disability as set forth in our standard form of Unit Forfeiture Agreement. |
At the effective time of this offering, we intend to implement a compensation program for our non-employee directors under which each non-employee director will receive the following amounts for their service on our board of directors:
| • | at each annual meeting of stockholders, a number of shares of restricted stock valued at $ as of the date of grant, which will vest in a single installment on the earliest of the first anniversary of the date of grant, the next annual meeting of stockholders and a change in control of us; |
| • | an annual retainer of $ ; and |
| • | if the director serves on a committee of our board of directors, an additional annual retainer as follows: |
| • | chairman of the audit committee: $ ; |
| • | audit committee member other than the chairman: $ ; |
| • | chairman of the compensation committee: $ ; |
| • | compensation committee member other than the chairman: $ ; |
| • | chairman of the nominating and corporate governance committee: $ ; and |
| • | nominating and corporate governance committee member other than the chairman: $ . |
Annual retainers will be payable in arrears in four equal quarterly installments not later than the 15th day following the end of each fiscal quarter and prorated for any portion of a quarter that a director is not serving as a non-employee member of our board. No retainer will be paid under the program for service prior to the program’s effectiveness.
Each member of our board of directors is entitled to be reimbursed for reasonable travel and other expenses incurred in connection with attending meetings of the board of directors and any committee of the board of directors on which he or she serves.
163
Table of Contents
CERTAIN RELATIONSHIPS AND RELATED PARTY TRANSACTIONS
Other than compensation agreements and other arrangements which are described under “Executive and Director Compensation” and the transactions described below, since January 1, 2016, there has not been, and there is not currently proposed, any transaction or series of similar transactions to which we were or will be a party in which the amount involved exceeded or will exceed $120,000 and in which any of our directors, executive officers or holders of more than 5% of our capital stock, or 5% Security Holders, or an affiliate or family member thereof, had or will have a direct or indirect material interest.
Operating Agreement of Electrocore, LLC
We are party to the Operating Agreement with our current members. The Operating Agreement, which contains provisions relating to membership interests and the right of our members to appoint the members to our board of directors, will terminate upon the closing of this offering. See “Management—Board Composition.”
Series A Equity Issuances
In March 2016, we consummated a final closing of our Series A financing pursuant to which we issued approximately 3.0 million Series A Preferred Units at an issue price of $0.85 per unit, or approximately $2.6 million in the aggregate. In connection with such closing, GHI, a 5% Security Holder, purchased approximately 1.0 million Series A Preferred Units for $0.9 million and CV II, a 5% Security Holder, purchased approximately 2.0 million Series A Preferred Units for approximately $1.7 million, including amounts converted pursuant to a term loan conversion as described below. In addition, CV II exercised an outstanding warrant and acquired approximately 2.3 million Series A Preferred Units for $1.7 million. Dr. Rubin, one of our directors, serves as a Managing Director of GHI. Mr. Errico and Dr. Errico, two of our directors, have a pecuniary interest in, serve as managers of, and have voting control over CV II.
Term Loan Conversion
In December 2015, CV II loaned us $1.25 million pursuant to a Loan and Security Agreement. In connection with this loan, we issued 66,177 warrants to CV II to purchase Series A Preferred Units at an exercise price of $0.85 per unit. These warrants expire on December 22, 2025. Pursuant to the terms of this loan, CV II elected to convert the term loan of $1.25 million and related accrued interest of $49,935 into approximately 1.5 million Series A Preferred Units in two installments in March 2016 and September 2016 at a price of $0.85 per Unit.
Bridge Financing
Beginning in June 2016, we commenced a note and warrant financing, or the Bridge Financing, pursuant to which we issued to investors a convertible promissory note, or Bridge Note, with annual interest of 10%. Each investor in the Bridge Financing was also issued a warrant, or Bridge Warrant, to purchase a number of shares issued in our next Qualified Equity Financing, or the Next Round Securities, equal to 20% of the original principal amount of the investor’s Bridge Note divided by the purchase price payable for such equity securities in the Qualified Equity Financing, or the Next Round Price. The Bridge Notes, together with all accrued interest, were automatically convertible upon the closing of the Qualified Equity Financing into the Next Round Securities at a per share price equal to 90% of the Next Round Price, or optionally convertible at any time at the holder’s option into our Series A Preferred Units at a price of $0.85 per unit.
ECNG is a limited liability company in which Mr. Errico and Dr. Errico have a pecuniary interest, which they serve as managers and over which they have voting control. In June and July 2016, ECNG purchased in the aggregate $1.5 million in Bridge Notes. In September 2016, ECNG converted approximately $1.5 million in principal and accrued interest under its Bridge Notes into approximately 1.8 million Series A Preferred Units.
164
Table of Contents
Following the Bridge Note conversion noted above, the terms of the Bridge Financing were amended to provide that future investors in the Bridge Financing were entitled to receive, in addition to their Bridge Note and Bridge Warrant, up to two Common Units for each dollar invested in the Bridge Financing.
From September 2016 through June 2017, we raised approximately $25.6 million from the issuance of additional Bridge Notes and issued approximately 41.9 million Common Units. Of these amounts, CV II purchased approximately $16.9 million in Bridge Notes and was issued approximately 33.7 million Common Units.
Series B Financing
Commitment Letter. In July 2017, CV II, GHI, Mr. Tullis, one of our directors, and TOP II, an entity for which Mr. Tullis serves as the managing partner of its general partner, entered into a commitment letter with us pursuant to which such investors agreed, among other things, to invest in the aggregate approximately $9 million in the initial closing of our Series B Preferred Unit financing and to consent to certain amendments to our Operating Agreement. In exchange for such commitments, the investors were issued two Common Units for each dollar committed. The table below summarizes these issuances.
| Investor |
Series B Commitment Amount |
Common Units Issued |
||||||
| GHI |
$ | 5,000,000 | 10,000,000 | |||||
| CV II |
$ | 3,870,000 | 7,740,000 | |||||
| James L.L. Tullis(1) |
$ | 300,000 | 600,000 | |||||
|
|
|
|
|
|||||
| $ | 9,170,000 | 18,340,000 | ||||||
|
|
|
|
|
|||||
| (1) | Includes amounts for TOP II. |
Series B Recapitalization. In August 2017, in connection with the initial closing of our Series B Preferred Unit financing, among other things, (i) the holders of our Series A Preferred Units agreed to eliminate approximately $54.9 million in liquidation preference in exchange for the issuance to such holders of approximately 46.9 million Common Units, and (ii) the holders of Common Units that were entitled to approximately $30.9 million in liquidation preference agreed to eliminate such preference in exchange for the issuance to such holders of approximately 26.4 million Common Units. The table below summarizes the issuances to certain related parties in connection with this recapitalization.
| Member |
Common Units Issued in Series B Recapitalization |
|||
| GHI |
15,384,615 | |||
| CV II (1) |
32,818,632 | |||
| ECNG, LLC |
1,304,356 | |||
| James L.L. Tullis (2) |
2,042,308 | |||
| (1) | Includes units issued for the benefit of Mr. Errico, Dr. Errico and Mrs. Theofilos, and their affiliates. |
| (2) | Includes units issued to TOP II and Mr. Tullis’ spouse and family, and trusts for the benefit of his spouse and family. |
Initial Series B Closing. In August 2017, we consummated the initial closing of our Series B Preferred Unit financing pursuant to which we issued approximately 51.1 million Series B Preferred Units for approximately $35.8 million in the aggregate. Each investor in our Series B financing was issued Series B Preferred Units at a price of $0.70 per unit, together with a warrant, or Series B Common Warrant, to purchase a number of our Common Units equal to 50% of the original issue price of the Series B
165
Table of Contents
Preferred Units purchased by such investor in our Series B Preferred Unit financing, divided by $1.25. The exercise price for the Common Units purchasable pursuant to the Series B Common Warrants is $1.25 per unit and the Series B Common Warrants have a five-year term; provided that the Series B Common Warrants will expire upon the closing of this offering, if not previously exercised. The table below summarizes the issuances at our initial Series B closing to certain related parties.
| Purchaser |
Series B Investment Amount |
Series B Units Purchased |
Common Units Underlying Series B Common Warrants |
|||||||||
| GHI |
$ | 5,000,000 | 7,142,858 | 2,000,000 | ||||||||
| CV II (1) |
$ | 21,530,416 | * | 30,757,737 | 8,612,166 | |||||||
| ECNG, LLC |
$ | 990,463 | 1,414,947 | 396,185 | ||||||||
| James L.L. Tullis (2) |
$ | 300,000 | 428,572 | 120,000 | ||||||||
| (1) | Includes the conversion of approximately $17.7 million in principal and accrued interest under outstanding Bridge Notes. |
| (2) | Includes amounts for TOP II. |
Additional Series B Closings. From August through November 2017, we consummated additional closings under our Series B financing pursuant to which we issued in the aggregate an additional approximately 54.0 million Series B Preferred Units at an issue price of $0.70 per unit, or approximately $37.8 million in the aggregate. In connection with such closings, certain related parties purchased Series B Preferred Units. Each investor in our additional Series B closings was issued a Series B Common Warrant in the form of the initial Series B Preferred Unit closing, except that the terms of the Series B Preferred Units financing were amended to provide that for any investor who, together with its affiliates, purchased not less than $15.0 million of Series B Preferred Units (excluding amounts purchased at the initial Series B closing), the Series B Common Warrant coverage amount for such investor was increased from 50% to 100%. The table below summarizes the issuances at our additional Series B closings to certain related parties.
| Series B Investment Amount |
Series B Preferred Units Purchased |
Common Units Underlying Series B Common Warrants |
||||||||||
| Purchaser |
||||||||||||
| American Investment Holdings(1) |
$ | 11,000,000 | 15,714,286 | 8,800,000 | ||||||||
| Vinik Family Foundation(1) |
$ | 4,000,000 | 5,714,286 | 3,200,000 | ||||||||
| CV II |
$ | 8,400,000 | 12,000,000 | 3,360,000 | ||||||||
| (1) | American Investment Holdings and Vinik Family Foundation are affiliates of Mr. Vinik, who served as one of our directors during 2017. |
Investor Rights Agreement
Pursuant to the terms of our Amended and Restated Investor Rights Agreement, certain holders of our units, including CV II, GHI, ECNG, TOP II, Mr. Errico, Dr. Errico, Mrs. Theofilos, and certain of their affiliates, are entitled to certain demand and piggyback registration rights with respect to our securities held by them, certain information and observer rights, and certain additional rights. Certain provisions of the investor rights agreement will terminate in connection with this offering. See “Description of Capital Stock” for additional information.
Conversion to Corporate Form
Prior to the closing of this offering, we will convert from a Delaware limited liability company to a Delaware corporation under the name electroCore, Inc. Existing holders, including our 5% Security
166
Table of Contents
Holders, executive officers and directors, of our Common Units, Series A Preferred Units and Series B Preferred Units, and warrants to purchase our Units, will receive the number of shares of common stock, the number of warrants, and the number of options, respectively, described in this prospectus as a result of the corporate conversion. The existing securities held by our officers, directors, nominees for director and 5% Security Holders, executive officers and directors will be converted on the same basis as all other holders of such securities. See “Corporate Conversion” and “Principal Stockholders” for additional information.
The following table details the number of Profits Interests held by each of our executive officers and the number of shares of common stock and options each executive officer will receive as a result of the conversion of these Profits Interest in the corporation conversion.
| Name |
Profits Interest |
Shares of common stock upon corporate conversion |
Options granted upon corporate conversion | |||
| Francis R. Amato |
16,832,573 | |||||
| Joseph P. Errico |
11,901,715 | |||||
| Glenn S. Vraniak |
4,360,858 | |||||
| Peter S. Staats, M.D. |
4,380,000 |
Limitation of Liability and Indemnification
As permitted by Delaware law, we intend to adopt provisions in our certificate of incorporation, which will be effective as of the closing date of this offering, that limit or eliminate the personal liability of our directors. Our certificate of incorporation will limit the liability of directors to the maximum extent permitted by Delaware law. Delaware law provides that directors of a corporation will not be personally liable for monetary damages for breaches of their fiduciary duties as directors, except liability for:
| • | any breach of the director’s duty of loyalty to us or our stockholders; |
| • | any act or omission not in good faith or that involves intentional misconduct or a knowing violation of law; |
| • | any unlawful payments related to dividends or unlawful stock repurchases, redemptions or other distributions; or |
| • | any transaction from which the director derived an improper personal benefit. |
These limitations do not apply to liabilities arising under federal securities laws and do not affect the availability of equitable remedies, including injunctive relief or rescission. If Delaware law is amended to authorize the further elimination or limiting of a director, then the liability of our directors will be eliminated or limited to the fullest extent permitted by Delaware law as so amended.
As permitted by Delaware law, our certificate of incorporation that will be effective as of the closing date of this offering will also provide that:
| • | we will indemnify our directors and officers to the fullest extent permitted by law; |
| • | we may indemnify our other employees and other agents to the same extent that we indemnify our officers and directors, unless otherwise determined by our board of directors; and |
| • | we will advance expenses to our directors and officers in connection with legal proceedings in connection with a legal proceeding to the fullest extent permitted by law. |
167
Table of Contents
We anticipate entering into indemnification agreements with our directors and officers to provide such officers and directors with additional contractual assurances regarding the scope of their indemnification. We expect that each of these indemnification agreements will provide that we will indemnify the director or officer to the fullest extent permitted by law for claims arising in his capacity as a director or officer, provided that he acted in good faith and in a manner that he reasonably believed to be in, or not opposed to, our best interests and, with respect to any criminal proceeding, had no reasonable cause to believe that his conduct was unlawful. We expect that each of these indemnification agreements will provide that in the event that we do not assume the defense of a claim against a director or officer, we will be required to advance his expenses in connection with his defense, provided that he undertakes to repay all amounts advanced if it is ultimately determined that he is not entitled to be indemnified by us.
We also intend to purchase and maintain insurance on behalf of any person who is or was a director or officer against any loss arising from any claim asserted against him or her and incurred by him or her in any such capacity, subject to certain exclusions.
We believe that these provisions and agreements are necessary to attract and retain qualified persons as directors and officers. Insofar as indemnification for liabilities arising under the Securities Act may be permitted to directors, officers or persons controlling our company pursuant to the foregoing provisions, we understand that in the opinion of the SEC such indemnification is against public policy as expressed in the Securities Act and is therefore unenforceable.
Policies and Procedures with Respect to Related Party Transactions
In accordance with the charter of our audit committee, which will become effective upon the closing of this offering, and our policy on related party transactions, which our board of directors will adopt in connection with this offering, our audit committee will be responsible for reviewing and approving related party transactions. The related party transaction policy will apply to transactions, arrangements and relationships where the aggregate amount involved will or may be expected to exceed $120,000 in any calendar year, where we are a participant and in which a related person has or will have a direct or indirect material interest. A related person is: (1) any of our directors, nominees for director or executive officers; (2) any immediate family member of a director, nominee for director or executive officer; and (3) any person, and his or her immediate family members, or entity that was a beneficial owner of 5% or more of any of our outstanding equity securities at the time the transaction occurred or existed.
In the course of its review and approval of related party transactions, our audit committee will consider the relevant facts and circumstances to decide whether to approve such transactions. Our audit committee will approve only those transactions that it determines are in our best interest. In particular, our policy on related party transactions will require our audit committee to consider, among other factors it deems appropriate:
| • | whether the related party transaction is on terms no less favorable than terms generally available to an unaffiliated third party under the same or similar circumstances; and |
| • | the extent of the related party’s interest in the transaction. |
Pursuant to our policy on related party transactions, our audit committee will identify the following categories of transactions as deemed to be preapproved by the audit committee, even if the aggregate amount involved exceeds the $120,000 threshold:
| • | our employment of any executive officer or compensation paid by us to any executive officer if our compensation committee approved (or recommended that our board of directors approve) such compensation; |
| • | any compensation paid to a director if the compensation is required to be reported in our proxy statement under Item 402 of the SEC’s compensation disclosure requirements; |
168
Table of Contents
| • | any transaction with another company at which a related person’s only relationship is as an employee (other than an executive officer), director or beneficial owner of less than 10% of that company’s shares, if the aggregate amount involved does not exceed the greater of $1.0 million, or 2% of that company’s total annual net product revenues; |
| • | any charitable contribution, grant or endowment made by us to a charitable organization, foundation or university at which a related person’s only relationship is as an employee (other than an executive officer) or a director, if the aggregate amount involved does not exceed the lesser of $1.0 million, or 2% of the charitable organization’s total annual receipts; |
| • | any transaction where the related person’s interest arises solely from the ownership of our common stock and all holders of our common stock received the same benefit on a pro rata basis; |
| • | any transaction involving a related person where the rates or charges involved are determined by competitive bids; |
| • | any transaction with a related person involving the rendering of services as a common or contract carrier, or public utility, at rates or charges fixed in conformity with law or governmental authority; and |
| • | any transaction with a related person involving services as a bank depositary of funds, transfer agent, registrar, trustee under a trust indenture, or similar services. |
In addition, our code of business conduct and ethics, which will become effective upon the closing of this offering, requires that each of our employees and directors inform his or her superior or the chairman of the audit committee, respectively, of any material transaction or relationship that comes to their attention that could reasonably be expected to create a conflict of interest. Further, at least annually, each director and executive officer will complete a detailed questionnaire that asks questions about any business relationship that may give rise to a conflict of interest and all transactions in which we are involved and in which the executive officer, a director or a related person has a direct or indirect material interest.
169
Table of Contents
The following table sets forth information as of , 2018 regarding the beneficial ownership of our common stock, giving pro forma effect to our conversion from a Delaware limited liability company to a Delaware corporation, by:
| • | each person or group who is known by us to beneficially own more than 5% of our outstanding shares of common stock; |
| • | each of our executive officers; |
| • | each of our directors; and |
| • | all of our executive officers and directors as a group. |
Beneficial ownership for the purposes of the following table is determined in accordance with the rules and regulations of the SEC. These rules generally provide that a person is the beneficial owner of securities if such person has or shares the power to vote or direct the voting of securities, or to dispose or direct the disposition of securities or has the right to acquire such powers within 60 days. For purposes of calculating each person’s percentage ownership, common stock issuable pursuant to options exercisable within 60 days are included as outstanding and beneficially owned for that person or group, but are not deemed outstanding for the purposes of computing the percentage ownership of any other person. Except as disclosed in the footnotes to this table and subject to applicable community property laws, we believe that each beneficial owner identified in the table possesses sole voting and investment power over all common stock shown as beneficially owned by the beneficial owner.
The percentage of beneficial ownership is based on shares of common stock outstanding prior to this offering after giving effect to our conversion from a Delaware limited liability company to a Delaware corporation, shares of common stock to be outstanding after the completion of this offering, assuming no exercise of the underwriters’ option to purchase additional shares of our common stock and shares of common stock to be outstanding after the completion of this offering, assuming exercise of the underwriters’ option to purchase additional shares of our common stock in full. The percentage of beneficial ownership further assumes that the corporate conversion had occurred on , based on the assumed initial public offering price of $ per share (the midpoint of the price range set forth on the cover page of this prospectus).
The number of shares of common stock, and the number of shares of common stock subject to options, of electroCore, Inc. that holders of our Profits Interest will receive in the corporate conversion will vary depending on the initial public offering price set forth on the cover page of this prospectus. See “Corporate Conversion” for additional information.
170
Table of Contents
Unless otherwise indicated in the table or footnotes below, the address for each beneficial owner is c/o Electrocore, LLC, 150 Allen Road, Suite 201, Basking Ridge, New Jersey 07920.
| After this offering | ||||||||||||||||||||||||
| Prior to this offering | Assuming underwriters’ option to purchase additional shares is not exercised |
Assuming underwriters’ option to purchase additional shares is exercised in full |
||||||||||||||||||||||
| Number of Shares beneficially owned |
Number of shares beneficially owned |
Number of shares beneficially owned |
||||||||||||||||||||||
| Name |
Number of Shares |
Percentage of Shares |
Number of shares |
Percentage of shares |
Number of shares |
Percentage of shares |
||||||||||||||||||
| 5% or more stockholders |
||||||||||||||||||||||||
| Core Ventures II, LLC |
% | % | % | |||||||||||||||||||||
| Merck Global Health Innovation Fund, One Merck Drive 2W116 Whitehouse Station, NJ 08889 |
% | % | % | |||||||||||||||||||||
| Executive officers and directors |
||||||||||||||||||||||||
| Joseph P. Errico(1) |
% | % | % | |||||||||||||||||||||
| Francis R. Amato(2) |
% | % | % | |||||||||||||||||||||
| Glenn S. Vraniak(3) |
% | % | % | |||||||||||||||||||||
| Peter S. Staats, M.D.(4) |
% | % | % | |||||||||||||||||||||
| David Rubin, Ph.D.(5) |
% | % | % | |||||||||||||||||||||
| Jeffrey Vinik(6) |
% | % | % | |||||||||||||||||||||
| Nicholas Colucci(7) |
% | % | % | |||||||||||||||||||||
| Thomas J. Errico, M.D.(8) |
% | % | % | |||||||||||||||||||||
| Trevor Moody(9) |
% | % | % | |||||||||||||||||||||
| Kathryn Theofilos(10) |
% | % | % | |||||||||||||||||||||
| James L.L. Tullis(11) |
% | % | % | |||||||||||||||||||||
| Executive officers and directors as a group ( persons) |
% | % | % | |||||||||||||||||||||
| * | Represents less than 1%. |
| (1) | Includes (i) shares held directly by Mr. Errico and shares held by Mr. Errico’s spouse, children and trusts for the benefit of Mr. Errico’s spouse and children, (ii) shares held for the benefit of Mr. Errico indirectly by CV II and other entities, and (iii) shares of common stock which may be acquired upon the exercise of stock options which have vested or will vest within 60 days of the filing of this prospectus. Also includes shares held by CV II and other entities (the “Other Entities”) for the benefit of persons other than Mr. Errico. Mr. Errico serves as a manager of CV II and the Other Entities and has or shares voting control over such shares. |
| (2) | Includes (i) shares held directly by Mr. Amato, (ii) shares held for the benefit of Mr. Amato indirectly by CV II, and (iii) shares of common stock which may be acquired upon the exercise of stock options which have vested or will vest within 60 days of the filing of this prospectus. |
| (3) | Includes (i) shares held directly by Mr. Vraniak, and (ii) shares of common stock which may be acquired upon the exercise of stock options which have vested or will vest within 60 days of the filing of this prospectus. |
| (4) | Includes (i) shares held directly by Dr. Staats and his spouse, (ii) shares held by Prand Enterprises, LLC, (iii) shares held for the benefit of Prand Enterprises, LLC indirectly by CV II and the Other Entities, and (iv) shares of common stock which may be acquired upon the exercise of stock options which have vested or will vest within 60 days of the filing of this prospectus. |
| (5) | Dr. Rubin is the managing director of Merck GHI, but does not have nor share voting power with respect to shares of our capital stock owned by Merck GHI. |
| (6) | Represents (i) shares held directly by American Investment Holdings, LLC and (ii) shares held directly by the Vinik Family Foundation. |
| (7) | Includes (i) shares held directly by Mr. Colucci, (ii) shares held for the benefit of Mr. Colucci indirectly by CV II and the Other Entities, and (iii) shares of common stock which may be acquired upon the exercise of stock options which have vested or will vest within 60 days of the filing of this prospectus. |
| (8) | Includes (i) shares held directly by Dr. Errico and shares held by trusts for the benefit of Dr. Errico’s family members, (ii) shares held for the benefit of Dr. Errico indirectly by CV II and the Other Entities, and (iii) shares of common stock which may be acquired upon the exercise of stock options which have vested or will vest within 60 days of the filing of this prospectus. Also includes shares held by CV II and the Other Entities for the benefit of persons |
171
Table of Contents
| other than Dr. Errico. Dr. Errico serves as a manager of CV II and the Other Entities and has or shares voting control over such shares. |
| (9) | Includes (i) shares held directly by Mr. Moody, and (ii) shares of common stock which may be acquired upon the exercise of stock options which have vested or will vest within 60 days of the filing of this prospectus. |
| (10) | Includes (i) shares held directly by Mrs. Theofilos and her children, (ii) shares held directly by a limited liability company affiliated with Mrs. Theofilos, and (iii) shares held for the benefit of Mrs. Theofilos indirectly by CV II and the Other Entities. |
| (11) | Represents (i) shares held directly by Mr. Tullis and shares held directly by his spouse and family trusts, (ii) shares held directly by Tullis Opportunity Fund II LP, and (iii) shares of common stock which may be acquired upon the exercise of stock options which have vested or will vest within 60 days of the filing of this prospectus. |
172
Table of Contents
The following description summarizes important terms of our capital stock. For a complete description, you should refer to our certificate of incorporation and bylaws, forms of which have been filed as exhibits to the registration statement of which this prospectus is a part, as well as the relevant portions of the DGCL. References to our certificate of incorporation and bylaws are to our certificate of incorporation and our bylaws, respectively, each of which will become effective upon completion of the corporate conversion that will occur prior to the closing of this offering. The description of our common stock and preferred stock reflects the completion of the corporate conversion that will occur prior to the closing of this offering.
General
Upon the closing of this offering, our authorized capital stock will consist of: (i) shares of common stock, par value $0.001 per share; and (ii) shares of preferred stock, par value $0.001 per share.
As of , 2018, we had outstanding shares of common stock, and approximately stockholders of record, after giving effect to the completion of the corporate conversion described above in the section entitled “Corporate Conversion.” Based on an assumed initial public offering price of $ (the midpoint of the range set forth on the cover page of this prospectus), upon completion of the corporate conversion and the closing of this offering, there will be shares of common stock outstanding and no shares of preferred stock outstanding.
Common Stock
Voting Rights
Each holder of our common stock will be entitled to one vote for each share on all matters submitted to a vote of the stockholders, including the election of directors. Under our certificate of incorporation and our amended and restated bylaws that will be in effect following the completion of this offering, our stockholders will not have cumulative voting rights. Because of this, the holders of a majority of the shares of common stock entitled to vote in any election of directors will be able to elect all of the directors standing for election, if they should so choose.
Dividend Rights
Subject to preferences that may be applicable to any then-outstanding preferred stock, holders of common stock will not be entitled to receive ratably those dividends, if any, as may be declared from time to time by the board of directors out of legally available funds.
Liquidation Rights
In the event of our liquidation, dissolution or winding up, holders of common stock will be entitled to share ratably in the net assets legally available for distribution to stockholders after the payment of all of our debts and other liabilities and the satisfaction of any liquidation preference granted to the holders of any then-outstanding shares of preferred stock.
Other Rights and Preferences
Holders of our common stock will have no preemptive, conversion or subscription rights and there will be no redemption or sinking fund provisions applicable to the common stock. The rights, preferences and privileges of the holders of common stock will be subject to, and may be adversely affected by, the rights of the holders of shares of any series of preferred stock that we may designate in the future.
173
Table of Contents
Preferred Stock
Following the corporate conversion and the completion of this offering, our board of directors will have the authority, without further action by our stockholders, to issue up to shares of preferred stock in one or more series, to establish from time to time the number of shares to be included in each such series, to fix the rights, preferences and privileges of the shares of each series and any qualifications, limitations or restrictions thereon, and to increase or decrease the number of shares of any such series, but not below the number of shares of such series then outstanding.
Our board of directors may authorize the issuance of preferred stock with voting or conversion rights that could adversely affect the voting power or other rights of the holders of our common stock. The purpose of authorizing our board of directors to issue preferred stock and determine its rights and preferences is to eliminate delays associated with a stockholder vote on specific issuances. The issuance of preferred stock, while providing flexibility in connection with possible acquisitions and other corporate purposes, could, among other things, have the effect of delaying, deferring or preventing a change of control of our company and may adversely affect the market price of our common stock and the voting and other rights of the holders of our common stock. It is not possible to state the actual effect of the issuance of any shares of preferred stock on the rights of holders of common stock until the board of directors determines the specific rights attached to that preferred stock.
We have no present plans to issue any shares of preferred stock.
Registration Rights
Under our Amended and Restated Investor Rights Agreement, following the consummation of this offering, the holders of approximately shares of common stock, or their transferees, will have the right to require us to register their shares under the Securities Act so that those shares may be publicly resold, or to include their shares in any registration statement we file, in each case as described below.
Demand Registration Rights
Based on the number of shares outstanding as of December 31, 2017, after the consummation of this offering, the holders of approximately shares of our common stock (on an as-converted basis), or their transferees, will be entitled to certain demand registration rights. Beginning one hundred eighty (180) days following the effectiveness of the registration statement of which this prospectus is a part, the holders of at least 55% of these shares can, on not more than three occasions, request that we register at least 40% of the shares issued to such holders, or a lesser percentage if the anticipated aggregate offering price, net of underwriting discounts and commissions, would exceed $5,000,000. Additionally, we will not be required to effect a demand registration during the period beginning 60 days prior to our good faith estimate of the filing of, and ending 180 days following the effectiveness of, a company-initiated registration statement relating to an initial public offering of our securities. These registration rights are further subject to specified conditions and limitations, including the right of the underwriters, if any, to limit the number of shares included in any such registration under specified circumstances. Upon such a request, we are required to use commercially reasonable efforts to effect the registration as soon as practicable.
Piggyback Registration Rights
Based on the number of shares outstanding as of December 31, 2017, after the consummation of this offering, in the event that we determine to register any of our securities under the Securities Act (subject to certain exceptions), either for our own account or for the account of other security holders, the holders of approximately shares of our common stock (on an as-converted basis), or their transferees, will be entitled to certain “piggyback” registration rights allowing the holders to include
174
Table of Contents
their shares in such registration, subject to certain marketing and other limitations. As a result, whenever we propose to file a registration statement under the Securities Act, other than with respect to a registration related to employee benefit plans, the offer and sale of debt securities, or corporate reorganizations or certain other transactions, the holders of these shares are entitled to notice of the registration and have the right, subject to limitations that the underwriters may impose on the number of shares included in the registration, to include their shares in the registration. In an underwritten offering, the managing underwriter, if any, has the right, subject to specified conditions, to limit the number of shares such holders may include.
Registration on Form S-3
Based on the number of shares outstanding as of December 31, 2017, after the consummation of this offering, the holders of approximately shares of our common stock (on an as-converted basis), or their transferees, will be entitled to certain Form S-3 registration rights. The holders of at least 20% of these shares can make a written request that we register their shares on Form S-3 if we are eligible to file a registration statement on Form S-3 and if the aggregate price to the public of the shares offered is at least $500,000 net of certain expenses related to the sale of the shares. These stockholders may make an unlimited number of requests for registration on Form S-3, but in no event shall we be required to file more than two registrations on Form S-3 within any 12-month period.
Expenses of Registration
We will pay all expenses relating to any demand, piggyback or Form S-3 registration, other than underwriting discounts and commissions, subject to specified conditions and limitations.
Termination of Registration Rights
The registration rights granted under the Amended and Restated Investor Rights Agreement will terminate, with respect to a particular holder, at the earlier of: (i) such time as that holder and its affiliates may sell all of their shares of common stock pursuant to Rule 144 under the Securities Act during any 90-day period; and (ii) the seven year anniversary of this offering.
Anti-Takeover Provisions
The provisions of Delaware law, and our certificate of incorporation and our bylaws could have the effect of delaying, deferring or discouraging another person from acquiring control of our company. These provisions, which are summarized below, may have the effect of discouraging takeover bids. They are also designed, in part, to encourage persons seeking to acquire control of us to negotiate first with our board of directors. We believe that the benefits of increased protection of our potential ability to negotiate with an unfriendly or unsolicited acquirer outweigh the disadvantages of discouraging a proposal to acquire us because negotiation of these proposals could result in an improvement of their terms.
Section 203 of the Delaware General Corporation Law
We are subject to Section 203 of the DGCL, which prohibits a Delaware corporation from engaging in any business combination with any interested stockholder for a period of three years after the date that such stockholder became an interested stockholder, with the following exceptions:
| • | before such date, the board of directors of the corporation approved either the business combination or the transaction that resulted in the stockholder becoming an interested stockholder; |
| • | upon completion of the transaction that resulted in the stockholder becoming an interested stockholder, the interested stockholder owned at least 85% of the voting stock of the |
175
Table of Contents
| corporation outstanding at the time the transaction began, excluding for purposes of determining the voting stock outstanding, but not the outstanding voting stock owned by the interested stockholder, those shares owned (i) by persons who are directors and also officers and (ii) employee stock plans in which employee participants do not have the right to determine confidentially whether shares held subject to the plan will be tendered in a tender or exchange offer; or |
| • | on or after such date, the business combination is approved by the board of directors and authorized at an annual or special meeting of the stockholders, and not by written consent, by the affirmative vote of at least 66 2/3% of the outstanding voting stock that is not owned by the interested stockholder. |
In general, Section 203 defines a “business combination” to include the following:
| • | any merger or consolidation involving the corporation and the interested stockholder; |
| • | any sale, transfer, pledge or other disposition of 10% or more of the assets of the corporation involving the interested stockholder; |
| • | subject to specified exceptions, any transaction that results in the issuance or transfer by the corporation of any stock of the corporation to the interested stockholder; |
| • | any transaction involving the corporation that has the effect of increasing the proportionate share of the stock or any class or series of the corporation beneficially owned by the interested stockholder; or |
| • | the receipt by the interested stockholder of the benefit of any loans, advances, guarantees, pledges or other financial benefits by or through the corporation. |
In general, Section 203 defines an “interested stockholder” as an entity or person who, together with the person’s affiliates and associates, beneficially owns, or within three years prior to the time of determination of interested stockholder status did own, 15% or more of the outstanding voting stock of the corporation.
Our Certificate of Incorporation and Bylaws
Our certificate of incorporation and bylaws will include a number of provisions that could deter hostile takeovers or delay or prevent changes in control of our company, including the following:
| • | Classified Board. Our certificate of incorporation will provide for our board of directors to be divided into three classes with staggered three-year terms. Only one class of directors will be elected at each annual meeting of our stockholders, with the other classes continuing for the remainder of their respective three-year terms. Because our stockholders do not have cumulative voting rights, stockholders holding a majority of the shares of common stock outstanding will be able to elect all of our directors. Our certificate of incorporation and our bylaws will also provide that directors may be removed by the stockholders only for cause upon the vote of 66 2/3% or more of our outstanding common stock. Furthermore, the authorized number of directors may be changed only by resolution of the board of directors, and vacancies and newly created directorships on the board of directors may, except as otherwise required by law or determined by the board, only be filled by a majority vote of the directors then serving on the board, even though less than a quorum. |
| • | Special Meetings of Stockholders and Stockholder Action by Written Consent. Our certificate of incorporation and bylaws will provide that all stockholder actions must be effected at a duly called meeting of stockholders and will eliminate the right of stockholders to act by written consent without a meeting. Our bylaws will also provide that only our |
176
Table of Contents
| chairman of the board, Chief Executive Officer (or if there is no Chief Executive Officer, the President) or the board of directors pursuant to a resolution adopted by a majority of the total number of authorized directors may call a special meeting of stockholders. |
| • | Advance Notice Requirements for Stockholder Proposals. Our bylaws will provide that stockholders seeking to present proposals before a meeting of stockholders, including the nomination of director candidates, must provide timely advance notice in writing, and will specify requirements as to the form and content of a stockholder’s notice. |
| • | Amendment to Certificate of Incorporation and Bylaws. Our certificate of incorporation and bylaws will provide that the stockholders cannot amend the provisions described above except by a vote of 66 2/3% or more of our outstanding common stock. |
The combination of these provisions will make it more difficult for our existing stockholders to replace our board of directors as well as for another party to obtain control of us by replacing our board of directors. Since our board of directors has the power to retain and discharge our officers, these provisions could also make it more difficult for existing stockholders or another party to effect a change in management. In addition, the authorization of undesignated preferred stock makes it possible for our board of directors to issue preferred stock with voting or other rights or preferences that could impede any attempt to effect a change of control of our company.
These provisions are intended to enhance the likelihood of continued stability in the composition of our board of directors and its policies and to discourage coercive takeover practices and inadequate takeover bids. These provisions are also designed to reduce our vulnerability to hostile takeovers and to discourage tactics that may be used in proxy fights. However, such provisions could have the effect of discouraging others from making tender offers for our shares and may have the effect of delaying changes in our control or management. As a consequence, these provisions may also inhibit fluctuations in the market price of our stock that could result from actual or rumored takeover attempts. We believe that the benefits of these provisions, including increased protection of our potential ability to negotiate with the proponent of an unfriendly or unsolicited proposal to acquire or restructure our company, outweigh the disadvantages of discouraging takeover proposals, because negotiation of takeover proposals could result in an improvement of their terms.
Choice of Forum
Our certificate of incorporation will provide that the Court of Chancery of the state of Delaware will be the exclusive forum for: any derivative action or proceeding brought on our behalf; any action asserting a breach of fiduciary duty; any action asserting a claim against us arising pursuant to the DGCL, our certificate of incorporation or our bylaws; or any action asserting a claim against us that is governed by the internal affairs doctrine. The enforceability of similar choice of forum provisions in some other companies’ certificates of incorporation has been challenged in legal proceedings, and it is possible that, in connection with any action, a court could find the choice of forum provisions contained in our certificate of incorporation to be inapplicable or unenforceable in such action.
Limitation of Liability and Indemnification
Our certificate of incorporation will provide that no director will be personally liable for monetary damages for breach of any fiduciary duty as a director, except with respect to liability:
| • | for any breach of the director’s duty of loyalty to us or our stockholders; |
| • | for acts or omissions not in good faith or that involve intentional misconduct or a knowing violation of law; |
| • | under Section 174 of the DGCL (governing distributions to stockholders); or |
| • | for any transaction from which the director derived any improper personal benefit. |
177
Table of Contents
If the DGCL is amended to authorize corporate action further eliminating or limiting the personal liability of directors, then the liability of our directors will be eliminated or limited to the fullest extent permitted by the DGCL, as so amended. The modification or repeal of this provision of our certificate of incorporation will not adversely affect any right or protection of a director existing at the time of such modification or repeal.
Our bylaws will also provide that we will, to the fullest extent permitted by law, indemnify our directors and officers against all liabilities and expenses in any suit or proceeding or arising out of their status as an officer or director or their activities in these capacities. We will also indemnify any person who, at our request, is or was serving as a director, officer, employee, agent or trustee of another corporation or of a partnership, limited liability company, joint venture, trust or other enterprise. We may, by action of our board of directors, provide indemnification to our employees and agents within the same scope and effect as the foregoing indemnification of directors and officers.
Transfer Agent and Registrar
The transfer agent and registrar for our common stock will be .
Stock Exchange Listing
We intend to apply to list our common stock on the Nasdaq Global Select Market under the symbol “ECOR.”
178
Table of Contents
SHARES ELIGIBLE FOR FUTURE SALE
Prior to this offering, there has not been a public market for shares of our common stock, and we cannot predict the effect, if any, that market sales of shares of our common stock or the availability of shares of our common stock for sale will have on the market price of our common stock prevailing from time to time. Nevertheless, sales of substantial amounts of our common stock, including shares issued upon exercise of outstanding options, in the public market following this offering could adversely affect market prices prevailing from time to time and could impair our ability to raise capital through the sale of our equity securities.
Based upon the number of shares of our common stock outstanding as of December 31, 2017, and after giving effect to the corporate conversion, based on the assumed initial public offering price of $ (the midpoint of the price range set forth on the cover page of this prospectus) we will have shares of common stock outstanding upon the closing of this offering. Of these outstanding shares, all of the shares of common stock sold in this offering will be freely tradable, except that any shares purchased in this offering by our affiliates, as that term is defined in Rule 144 under the Securities Act, would only be able to be sold in compliance with the Rule 144 limitations described below.
The remaining outstanding shares of our common stock will be deemed “restricted securities” as defined in Rule 144. Restricted securities may be sold in the public market only if they are registered under the Securities Act or if they qualify for an exemption from registration under Rule 144 or Rule 701 promulgated under the Securities Act, which rules are summarized below. In addition, all of our security holders have entered into market standoff agreements with us or lock-up agreements with the underwriters under which they have agreed, subject to specific exceptions, not to sell any of our stock for at least 180 days following the date of this prospectus, as described below. As a result of these agreements and the provisions of our amended and restated investors’ rights agreement described above under “Description of Capital Stock—Registration Rights,” subject to the provisions of Rule 144 or Rule 701, shares will be available for sale in the public market as follows:
| • | beginning on the date of this prospectus, all of the shares sold in this offering will be immediately available for sale in the public market (except as described above); and |
| • | beginning 181 days after the date of this prospectus, additional shares will become eligible for sale in the public market, of which shares will be held by affiliates and subject to the volume and other restrictions of Rule 144, as described below. |
Lock-Up and Market Standoff Agreements
All of our directors, executive officers and our security holders are subject to lock-up agreements or market standoff provisions that, subject to certain exceptions, prohibit them from directly or indirectly offering, pledging, selling, contracting to sell, selling any option or contract to purchase, purchasing any option or contract to purchase, granting any option, right or warrant to purchase or otherwise transferring or disposing of any shares of our common stock, options to acquire shares of our common stock or any securities convertible into or exercisable or exchangeable for common stock, whether now owned or hereafter acquired, or entering into any swap or any other agreement or any transaction that transfer, in whole or in part, directly or indirectly, the economic consequence of ownership, for a period of 180 days following the date of this prospectus, without the prior written consent of Piper Jaffray & Co. and Evercore Group L.L.C. See the section entitled “Underwriting.”
Rule 144
In general, under Rule 144 as currently in effect, once we have been subject to public company reporting requirements for at least 90 days, a person who is not deemed to have been one of our affiliates for purposes of the Securities Act at any time during the 90 days preceding a sale and who has beneficially
179
Table of Contents
owned the shares proposed to be sold for at least six months, including the holding period of any prior owner other than our affiliates, is entitled to sell those shares without complying with the manner of sale, volume limitation or notice provisions of Rule 144, subject to compliance with the public information requirements of Rule 144. If such a person has beneficially owned the shares proposed to be sold for at least one year, including the holding period of any prior owner other than our affiliates, then that person would be entitled to sell those shares without complying with any of the requirements of Rule 144.
In general, under Rule 144, as currently in effect, our affiliates or persons selling shares on behalf of our affiliates are entitled to sell upon expiration of the lock-up and market standoff agreements described above, within any three-month period, a number of shares that does not exceed the greater of:
| • | 1% of the number of shares of our common stock then outstanding, which will equal approximately shares immediately after this offering; or |
| • | the average weekly trading volume of our common stock during the four calendar weeks preceding the filing of a notice on Form 144 with respect to that sale. |
Sales under Rule 144 by our affiliates or persons selling shares on behalf of our affiliates are also subject to certain manner of sale provisions and notice requirements and to the availability of current public information about us.
Rule 701
Rule 701 generally allows a stockholder who purchased shares of our common stock pursuant to a written compensatory plan or contract and who is not deemed to have been an affiliate of our company during the immediately preceding 90 days to sell these shares in reliance upon Rule 144, but without being required to comply with the public information, holding period, volume limitation or notice provisions of Rule 144. Rule 701 also permits affiliates of our company to sell their Rule 701 shares under Rule 144 without complying with the holding period requirements of Rule 144. All holders of Rule 701 shares, however, are required by that rule to wait until 90 days after the date of this prospectus before selling those shares pursuant to Rule 701 and are subject to the lock-up and market standoff agreements described above.
Stock Options
In connection with this offering, we intend to file a registration statement on Form S-8 under the Securities Act covering all of the shares of our common stock subject to outstanding options and the shares of our common stock reserved for issuance under our stock plans. We expect to file this registration statement as soon as permitted under the Securities Act. However, the shares registered on Form S-8 may be subject to the volume limitations and the manner of sale, notice and public information requirements of Rule 144 and will not be eligible for resale until expiration of the lock-up and market standoff agreements to which they are subject.
Registration Rights
We have granted demand, piggyback and Form S-3 registration rights to certain of our stockholders to sell our common stock. Registration of the sale of these shares under the Securities Act would result in these shares becoming freely tradable without restriction under the Securities Act immediately upon the effectiveness of the registration, except for shares purchased by affiliates. For a further description of these rights, see “Description of Capital Stock—Registration Rights.”
180
Table of Contents
CERTAIN MATERIAL U.S. FEDERAL INCOME AND ESTATE TAX CONSIDERATIONS
FOR NON-U.S. HOLDERS OF COMMON STOCK
The following is a general discussion of material U.S. federal income tax considerations and certain U.S. estate tax considerations relating to the ownership and disposition of our common stock applicable to non-U.S. holders. For purposes of this discussion, a “non-U.S. holder” means a beneficial owner of our common stock (other than an entity or arrangement that is treated as a partnership for U.S. federal income tax purposes) that is not, for U.S. federal income tax purposes, any of the following:
| • | an individual who is a citizen or resident of the United States; |
| • | a corporation (or other entity treated as a corporation for U.S. federal income tax purposes) created or organized in the United States or under the laws of the United States, any state thereof or the District of Columbia; |
| • | an estate, the income of which is includable in gross income for U.S. federal income tax purposes regardless of its source; or |
| • | a trust if (i) a court within the United States is able to exercise primary supervision over the administration of the trust and one or more “U.S. persons,” as defined under the U.S. Internal Revenue Code of 1986, as amended (which we refer to as the Code), have the authority to control all substantial decisions of the trust or (ii) such trust has made a valid election to be treated as a U.S. person for U.S. federal income tax purposes. |
This discussion is based on current provisions of the Code, final, temporary and proposed Treasury regulations promulgated thereunder (which we refer to as the Treasury Regulations), judicial decisions, published rulings and administrative pronouncements of the U.S. Internal Revenue Service, or IRS, all in effect as of the date of this prospectus and all of which are subject to change or to differing interpretation, possibly with retroactive effect. Any change could alter the tax consequences to non-U.S. holders described herein. There can be no assurance that the IRS, will not challenge one or more of the tax consequences described herein.
This discussion is limited to non-U.S. holders that hold our common stock as a “capital asset” within the meaning of Section 1221 of the Code (generally, property held for investment). This discussion does not address all aspects of U.S. federal income and estate taxation that may be relevant to a particular non-U.S. holder in light of that non-U.S. holder’s individual circumstances nor does it address any aspects of U.S. state, local or non-U.S. taxes, the alternative minimum tax, or the unearned income Medicare contribution tax on net investment income. This discussion also does not consider any specific facts or circumstances that may apply to a non-U.S. holder and does not address the special tax rules applicable to particular non-U.S. holders, such as:
| • | banks, insurance companies and other financial institutions; |
| • | brokers or dealers or traders in securities; |
| • | tax-exempt organizations; |
| • | pension plans; |
| • | persons who hold our common stock as part of a straddle, hedge, conversion transaction, synthetic security or other integrated investment or who have elected to mark securities to market; |
| • | “controlled foreign corporations,” “passive foreign investment companies,” and corporations that accumulate earnings to avoid U.S. federal income tax; |
| • | persons who hold or receive our common stock pursuant to the exercise of any employee stock option or otherwise as compensation; |
181
Table of Contents
| • | persons for whom our common stock constitutes “qualified small business stock” within the meaning of Section 1202 of the Code; |
| • | persons subject to special tax accounting rules as a result of any item of gross income with respect to our common stock being taken into account in an applicable financial statement; |
| • | non-U.S. governments; and |
| • | U.S. expatriates and former citizens or long-term residents of the United States. |
If a partnership (or other entity or arrangement treated as a partnership for U.S. federal income tax purposes) holds our common stock, the tax treatment of a partner therein will generally depend on the status of the partner and the activities of the partnership. Partners of a partnership holding our common stock should consult their tax advisors as to the particular U.S. federal income tax consequences applicable to them.
THIS SUMMARY IS NOT INTENDED TO CONSTITUTE A COMPLETE DESCRIPTION OF ALL TAX CONSEQUENCES FOR NON-U.S. HOLDERS RELATING TO THE OWNERSHIP AND DISPOSITION OF OUR COMMON STOCK. PROSPECTIVE HOLDERS OF OUR COMMON STOCK SHOULD CONSULT WITH THEIR TAX ADVISORS REGARDING THE TAX CONSEQUENCES TO THEM (INCLUDING THE APPLICATION AND EFFECT OF ANY STATE, LOCAL, NON-U.S. INCOME AND OTHER TAX LAWS) OF THE OWNERSHIP AND DISPOSITION OF OUR COMMON STOCK.
Distributions
As discussed under “Dividend Policy” above, we do not expect to make distributions on our common stock in the foreseeable future. However, if we do make distributions of cash or property on our common stock, such distributions will constitute dividends for U.S. federal income tax purposes to the extent paid from our current or accumulated earnings and profits, as determined under U.S. federal income tax principles. Amounts of distributions not treated as dividends for U.S. federal income tax purposes will first constitute a tax-free return of capital of the non-U.S. holder’s investment and be applied against and reduce a non-U.S. holder’s adjusted tax basis in its common stock, but not below zero. Any remaining excess will be treated as capital gain and will be treated as described below under “Gain on Sale or Other Disposition of Common Stock.” Any such distributions will also be subject to the discussions below under the headings “FATCA” and “Backup Withholding, Information Reporting and Other Reporting Requirements.”
Subject to the discussion in the next paragraph regarding effectively connected income, dividends paid to a non-U.S. holder generally will be subject to withholding of U.S. federal income tax at a 30% rate or such lower rate as may be specified by an applicable income tax treaty between the United States and such holder’s country of residence.
Dividends we pay to a non-U.S. holder that are effectively connected with its conduct of a trade or business within the United States (and, if required by an applicable tax treaty, are attributable to a U.S. permanent establishment or a fixed base maintained by such non-U.S. holder) will generally be exempt from the U.S. federal withholding tax, as described above, if the non-U.S. holder complies with applicable certification and disclosure requirements (generally including provision of a valid IRS Form W-8ECI (or applicable successor form) certifying that the dividends are effectively connected with the non-U.S. holder’s conduct of a trade or business within the United States). Instead, such dividends generally will be subject to U.S. federal income tax on a net income basis, at regular U.S. federal income tax rates as would apply if such holder were a U.S. person (as defined in the Code). Any U.S. effectively connected income received by a non-U.S. holder that is classified as a corporation for U.S. federal income tax purposes, may also be subject to an additional “branch profits tax” at a rate of 30% (or such lower rate as may be specified by an applicable income tax treaty).
182
Table of Contents
A non-U.S. holder of our common stock who claims the benefit of an applicable income tax treaty between the United States and such holder’s country of residence generally will be required to provide a properly executed IRS Form W-8BEN or W-8BEN-E (or successor form) and satisfy applicable certification and other requirements. Non-U.S. holders are urged to consult their tax advisors regarding their entitlement to benefits under a relevant income tax treaty and the specific methods available to them to satisfy these requirements.
Gain on Sale or Other Disposition of Common Stock
Subject to the discussion below under the headings “FATCA” and “Backup Withholding, Information Reporting and Other Reporting Requirements,” a non-U.S. holder generally will not be subject to U.S. federal income tax on any gain realized upon the sale or other disposition of the non-U.S. holder’s shares of common stock unless:
| • | the gain is effectively connected with a trade or business carried on by the non-U.S. holder within the United States (and, if required by an applicable income tax treaty, is attributable to a U.S. permanent establishment or fixed base maintained by such non-U.S. holder); |
| • | the non-U.S. holder is an individual and is present in the United States for 183 days or more in the taxable year of disposition and certain other conditions are met; or |
| • | we are or have been a “U.S. real property holding corporation” for U.S. federal income tax purposes at any time within the shorter of the five-year period preceding such disposition or such non-U.S. holder’s holding period of our common stock, and, provided that our common stock is regularly traded in an established securities market within the meaning of applicable Treasury Regulations, the non-U.S. holder has held, directly or constructively, at any time during said period, more than 5% of our common stock. |
Gain that is effectively connected with the conduct of a trade or business in the United States generally will be subject to U.S. federal income tax on a net income tax basis, at regular U.S. federal income tax rates. If the non-U.S. holder is a non-U.S. corporation, the branch profits tax described above also may apply to such effectively connected gain. An individual non-U.S. holder who is subject to U.S. federal income tax because the non-U.S. holder was present in the United States for 183 days or more during the year of sale or other disposition of our common stock will be subject to a flat 30% tax (or such lower rate as may be specified by an applicable income tax treaty) on the gain derived from such sale or other disposition, which may be offset by certain U.S. source capital losses, if any. We believe that we are not and we do not anticipate becoming a U.S. real property holding corporation for U.S. federal income tax purposes.
FATCA
The Foreign Account Tax Compliance Act, or FATCA, imposes a U.S. federal withholding tax of 30% on certain payments to foreign financial institutions, investment funds and certain other non-U.S. persons that fail to comply with certain information reporting and certification requirements pertaining to their direct and indirect U.S. securityholders and/or U.S. accountholders and are not otherwise exempt. Under applicable Treasury Regulations and IRS guidance, this withholding currently applies to payments of dividends, if any, on our common stock and will apply to payments of gross proceeds from a sale or other disposition of our common stock made on or after January 1, 2019. An intergovernmental agreement between the U.S. and an applicable foreign country may modify the requirements described in this paragraph. Prospective investors are encouraged to consult with their tax advisors regarding the possible implications of this legislation on their investment in our common stock.
Backup Withholding, Information Reporting and Other Reporting Requirements
We must report annually to the IRS and to each non-U.S. holder the amount of any distributions paid to, and the tax withheld with respect to, each non-U.S. holder. These reporting requirements apply
183
Table of Contents
regardless of whether withholding was reduced or eliminated by an applicable income tax treaty. Copies of this information reporting may also be made available under the provisions of a specific income tax treaty or agreement with the tax authorities in the country in which the non-U.S. holder resides or is established.
A non-U.S. holder will generally be subject to backup withholding for dividends on our common stock paid to such holder unless such holder certifies under penalties of perjury that, among other things, it is a non-U.S. holder (provided that the payor does not have actual knowledge or reason to know that such holder is a U.S. person) or otherwise establishes an exemption.
Information reporting and backup withholding generally will apply to the proceeds of a disposition of our common stock by a non-U.S. holder effected by or through the U.S. office of any broker, U.S. or non-U.S., unless the holder certifies its status as a non-U.S. holder and satisfies certain other requirements, or otherwise establishes an exemption. Generally, information reporting and backup withholding will not apply to a payment of disposition proceeds to a non-U.S. holder where the transaction is effected outside the United States through a non-U.S. office of a broker. However, for information reporting purposes, dispositions effected through a non-U.S. office of a broker with substantial U.S. ownership or operations generally will be treated in a manner similar to dispositions effected through a U.S. office of a broker. Non-U.S. holders should consult their tax advisors regarding the application of the information reporting and backup withholding rules to them.
Backup withholding is not an additional income tax. Any amounts withheld under the backup withholding rules from a payment to a non-U.S. holder generally can be credited against the non-U.S. holder’s U.S. federal income tax liability, if any, or refunded, provided that the required information is furnished to the IRS in a timely manner. Non-U.S. holders should consult their tax advisors regarding the application of the information reporting and backup withholding rules to them.
U.S. Federal Estate Tax
Shares of our common stock that are owned or treated as owned by an individual who is not a citizen or resident of the United States (as specially defined for U.S. federal estate tax purposes) at the time of death are considered U.S. situs assets and will be included in the individual’s gross estate for U.S. federal estate tax purposes. Such shares, therefore, may be subject to U.S. federal estate tax, unless an applicable estate tax or other treaty provides otherwise.
The preceding discussion of material U.S. federal income tax considerations and certain U.S. estate tax considerations is for information only. It is not legal or tax advice. Prospective investors should consult their tax advisors regarding the particular U.S. federal, state, local and non-U.S. tax consequences of owning and disposing of our common stock, including the consequences of any proposed changes in applicable laws.
184
Table of Contents
Piper Jaffray & Co. and Evercore Group L.L.C. are acting as representatives of each of the underwriters named below. Subject to the terms and conditions set forth in an underwriting agreement among us and the underwriters, we have agreed to sell to the underwriters, and each of the underwriters has agreed, severally and not jointly, to purchase from us, the number of shares of our common stock set forth opposite its name below.
| Underwriters | Number of Shares | |||
| Piper Jaffray & Co. |
||||
| Evercore Group L.L.C. |
||||
| JMP Securities LLC |
||||
|
|
|
|||
| Total |
||||
|
|
|
|||
Subject to the terms and conditions set forth in the underwriting agreement, the underwriters have agreed, severally and not jointly, to purchase all of the shares sold under the underwriting agreement if any of these shares are purchased. If an underwriter defaults, the underwriting agreement provides that the purchase commitments of the nondefaulting underwriters may be increased or the underwriting agreement may be terminated.
We have agreed to indemnify the several underwriters against certain liabilities, including liabilities under the Securities Act relating to losses or claims resulting from material misstatements in or omissions from this prospectus, the registration statement of which this prospectus is a part, certain free writing prospectuses that may be used in the offering and in any marketing materials used in connection with this offering and to contribute to payments the underwriters may be required to make in respect of those liabilities.
Discounts and Commissions
The representatives have advised us that the underwriters propose initially to offer the shares to the public at the public offering price set forth on the cover page of this prospectus and to dealers at that price less a concession not in excess of $ per share. After the initial offering, the public offering price, concession or any other term of this offering may be changed. The underwriters reserve the right to withdraw, cancel or modify offers to the public and to reject orders in whole or in part.
The following table shows the public offering price, underwriting discount and proceeds, before expenses, to us. The information assumes either no exercise or full exercise by the underwriters of their option to purchase additional shares.
| Per Share | Without Option |
With Option |
||||||||||
| Public Offering Price |
$ | $ | $ | |||||||||
| Underwriter Discount |
$ | $ | $ | |||||||||
| Proceeds, before expenses, to us |
$ | $ | $ | |||||||||
The estimated offering expenses payable by us, exclusive of the underwriting discount and commissions, are approximately $ million. We have also agreed to reimburse the underwriters for certain of their expenses in an amount not to exceed $ as set forth in the underwriting agreement.
The underwriting agreement provides that the obligations of the several underwriters to pay for and accept delivery of the shares of common stock offered by this prospectus are subject to the approval of certain legal matters by their counsel and to certain other conditions. The underwriters are obligated to
185
Table of Contents
take and pay for all of the shares of common stock offered by this prospectus if any such shares are taken. However, the underwriters are not required to take or pay for the shares covered by the underwriters’ option to purchase additional shares, described below. If an underwriter defaults, the underwriting agreement provides that the purchase commitments of the non-defaulting underwriters may be increased.
Option to Purchase Additional Shares
We have granted to the underwriters an option, exercisable for 30 days from the date of this prospectus, to purchase up to additional shares of common stock at the public offering price listed on the cover page of this prospectus, less the underwriting discount and commissions. The underwriters may exercise this option solely for the purpose of covering overallotments, if any, made in connection with the offering of the shares of common stock offered by this prospectus. To the extent the option is exercised, each underwriter will become obligated, subject to certain conditions, to purchase about the same percentage of the additional shares of common stock as the number listed next to the underwriter’s name in the table above bears to the total number of shares of common stock listed next to the names of all underwriters in the preceding table.
No Sales of Similar Securities
We, our executive officers and directors and substantially all of our other existing security holders have agreed not to sell or transfer any shares of our common stock or securities convertible into, exchangeable for, exercisable for, or repayable with shares of our common stock, for 180 days after the date of this prospectus without first obtaining the written consent of Piper Jaffray & Co. and Evercore Group L.L.C. Specifically, we and these other persons have agreed, with certain limited exceptions, not to directly or indirectly:
| • | offer, pledge, announce the intention to sell, sell or contract to sell any shares of our common stock; |
| • | sell any option or contract to purchase any shares of our common stock; |
| • | purchase any option or contract to sell any shares of our common stock; |
| • | grant any option, right or warrant to purchase any shares of our common stock; |
| • | dispose of or otherwise transfer any shares of our common stock; |
| • | demand that we file a registration statement related to our common stock; or |
| • | enter into any swap or other agreement that transfers, in whole or in part, the economic consequence of ownership of any shares of our common stock whether any such swap or transaction is to be settled by delivery of shares or other securities, in cash or otherwise. |
This lock-up provision applies to shares of our common stock and to securities convertible into or exchangeable or exercisable for or repayable with shares of our common stock. It also applies to shares of our common stock owned now or acquired later by the person executing the agreement or for which the person executing the agreement later acquires the power of disposition.
Listing
We intend to apply to list our common stock on The Nasdaq Global Select Market under the symbol “ECOR.” In order to meet the requirements for listing on that exchange, the underwriters have undertaken to sell a minimum number of shares to a minimum number of beneficial owners as required by that exchange.
186
Table of Contents
Before this offering, there has been no public market for our common stock. The initial public offering price will be determined through negotiations between us and the representatives. In addition to prevailing market conditions, the factors to be considered in determining the initial public offering price are:
| • | the valuation multiples of publicly traded companies that the representatives believe to be comparable to us; |
| • | our financial information; |
| • | the history of, and the prospects for, our company and the industry in which we compete; |
| • | an assessment of our management, its past and present operations and the prospects for, and timing of, our future net sales; |
| • | the present state of our development; and |
| • | the above factors in relation to market values and various valuation measures of other companies engaged in activities similar to ours. |
An active trading market for the shares may not develop. It is also possible that after this offering the shares will not trade in the public market at or above the initial public offering price.
The underwriters do not expect to sell more than 5% of the shares in the aggregate to accounts over which they exercise discretionary authority.
Price Stabilization, Short Positions and Penalty Bids
Until the distribution of the shares is completed, SEC rules may limit underwriters and selling group members from bidding for and purchasing shares of our common stock. However, the underwriters may engage in transactions that stabilize the price of our common stock, such as bids or purchases to peg, fix or maintain that price.
In connection with this offering, the underwriters may purchase and sell shares of our common stock in the open market. These transactions may include short sales, purchases on the open market to cover positions created by short sales and stabilizing transactions. Short sales involve the sale by the underwriters of a greater number of shares than they are required to purchase in this offering. “Covered” short sales are sales made in an amount not greater than the underwriters’ option to purchase additional shares described above. The underwriters may close out any covered short position by either exercising their option or purchasing shares in the open market. In determining the source of shares to close out the covered short position, the underwriters will consider, among other things, the price of shares available for purchase in the open market as compared to the price at which they may purchase shares through the overallotment option. “Naked” short sales are sales in excess of the overallotment option. The underwriters must close out any naked short position by purchasing shares in the open market. A naked short position is more likely to be created if the underwriters are concerned that there may be downward pressure on the price of our common stock in the open market after pricing that could adversely affect investors who purchase in this offering. Stabilizing transactions consist of various bids for or purchases of shares of our common stock made by the underwriters in the open market prior to the completion of this offering.
The underwriters may also impose a penalty bid. This occurs when a particular underwriter repays to the underwriters a portion of the underwriting discount received by it because the representatives have repurchased shares sold by or for the account of such underwriter in stabilizing or short covering transactions.
Similar to other purchase transactions, the underwriters’ purchases to cover the syndicate short sales may have the effect of raising or maintaining the market price of our common stock or preventing or
187
Table of Contents
retarding a decline in the market price of our common stock. As a result, the price of our common stock may be higher than the price that might otherwise exist in the open market. The underwriters may conduct these transactions on Nasdaq, in the over-the-counter market or otherwise.
Neither we nor any of the underwriters make any representation or prediction as to the direction or magnitude of any effect that the transactions described above may have on the price of our common stock. In addition, neither we nor any of the underwriters make any representation that the representatives will engage in these transactions or that these transactions, once commenced, will not be discontinued without notice.
Electronic Offer, Sale and Distribution of Shares
In connection with this offering, certain of the underwriters or securities dealers may distribute prospectuses by electronic means, such as e-mail. In addition, one or more of the underwriters may facilitate internet distribution for this offering to certain of their internet subscription customers. Any such underwriter may allocate a limited number of shares for sale to its online brokerage customers. An electronic prospectus is available on the internet websites maintained by any such underwriter. Other than the prospectus in electronic format, the information on the websites of any such underwriter is not part of this prospectus.
Other Relationships
The underwriters and their respective affiliates are full service financial institutions engaged in various activities, which may include securities trading, commercial and investment banking, financial advisory, investment management, investment research, principal investment, hedging, financing and brokerage activities. Certain of the underwriters and their affiliates have engaged in, and may in the future engage in, investment banking and other commercial dealings in the ordinary course of business with us or our affiliates. They have received, or may in the future receive, customary fees and commissions for these transactions.
In the ordinary course of their various business activities, the underwriters and their respective affiliates may make or hold a broad array of investments and actively trade debt and equity securities (or related derivative securities) and financial instruments (including bank loans) for their own account and for the accounts of their customers, and such investment and securities activities may involve securities and/or instruments of the issuer. The underwriters and their respective affiliates may also make investment recommendations and/or publish or express independent research views in respect of such securities or instruments and may at any time hold, or recommend to clients that they acquire, long and/or short positions in such securities and instruments.
Selling Restrictions
European Economic Area
In relation to each Member State of the European Economic Area which has implemented the Prospectus Directive (each, a “Relevant Member State”) an offer to the public of any shares of our common stock may not be made in that Relevant Member State, except that an offer to the public in that Relevant Member State of any shares of our common stock may be made at any time under the following exemptions under the Prospectus Directive, if they have been implemented in that Relevant Member State:
| (a) | to any legal entity which is a qualified investor as defined in the Prospectus Directive; |
| (b) | to fewer than 100 or, if the Relevant Member State has implemented the relevant provision of the 2010 PD Amending Directive, 150, natural or legal persons (other than qualified investors as defined in the Prospectus Directive), as permitted under the Prospectus Directive, subject to obtaining the prior consent of the representatives for any such offer; or |
188
Table of Contents
| (c) | in any other circumstances falling within Article 3(2) of the Prospectus Directive, provided that no such offer of shares of our common stock shall result in a requirement for the publication by us or any underwriter of a prospectus pursuant to Article 3 of the Prospectus Directive. |
For the purposes of this provision, the expression an “offer to the public” in relation to any shares of our common stock in any Relevant Member State means the communication in any form and by any means of sufficient information on the terms of the offer and any shares of our common stock to be offered so as to enable an investor to decide to purchase any shares of our common stock, as the same may be varied in that Member State by any measure implementing the Prospectus Directive in that Member State, the expression “Prospectus Directive” means Directive 2003/71/EC (and amendments thereto, including the 2010 PD Amending Directive, to the extent implemented in the Relevant Member State), and includes any relevant implementing measure in the Relevant Member State, and the expression “2010 PD Amending Directive” means Directive 2010/73/EU.
United Kingdom
Each underwriter has represented and agreed that:
| (a) | it has only communicated or caused to be communicated and will only communicate or cause to be communicated an invitation or inducement to engage in investment activity (within the meaning of Section 21 of the Financial Services and Markets Act 2000 (the “FSMA”)) received by it in connection with the issue or sale of the shares of our common stock in circumstances in which Section 21(1) of the FSMA does not apply to us; and |
| (b) | it has complied and will comply with all applicable provisions of the FSMA with respect to anything done by it in relation to the shares of our common stock in, from or otherwise involving the United Kingdom. |
Canada
The common stock may be sold only to purchasers purchasing as principal that are both “accredited investors” as defined in National Instrument 45-106 Prospectus and Registration Exemptions and “permitted clients” as defined in National Instrument 31-103 Registration Requirements, Exemptions and Ongoing Registrant Obligations. Any resale of the common shares must be made in accordance with an exemption from the prospectus requirements and in compliance with the registration requirements of applicable securities laws.
Hong Kong
The common stock may not be offered or sold in Hong Kong by means of any document other than (i) in circumstances which do not constitute an offer to the public within the meaning of the Companies Ordinance (Cap. 32, Laws of Hong Kong), or (ii) to “professional investors” within the meaning of the Securities and Futures Ordinance (Cap. 571, Laws of Hong Kong) and any rules made thereunder, or (iii) in other circumstances which do not result in the document being a “prospectus” within the meaning of the Companies Ordinance (Cap. 32, Laws of Hong Kong) and no advertisement, invitation or document relating to the shares may be issued or may be in the possession of any person for the purpose of issue (in each case whether in Hong Kong or elsewhere), which is directed at, or the contents of which are likely to be accessed or read by, the public in Hong Kong (except if permitted to do so under the laws of Hong Kong) other than with respect to common shares which are or are intended to be disposed of only to persons outside Hong Kong or only to “professional investors” within the meaning of the Securities and Futures Ordinance (Cap. 571, Laws of Hong Kong) and any rules made thereunder.
Singapore
This prospectus has not been registered as a prospectus with the Monetary Authority of Singapore.
189
Table of Contents
Accordingly, this prospectus and any other document or material in connection with the offer or sale, or invitation for subscription or purchase, of the common stock may not be circulated or distributed, nor may the common shares be offered or sold, or be made the subject of an invitation for subscription or purchase, whether directly or indirectly, to persons in Singapore other than (i) to an institutional investor under Section 274 of the Securities and Futures Act, Chapter 289 of Singapore (the “SFA”), (ii) to a relevant person pursuant to Section 275(1), or any person pursuant to Section 275(1A), and in accordance with the conditions specified in Section 275 of the SFA or (iii) otherwise pursuant to, and in accordance with the conditions of, any other applicable provision of the SFA, in each case subject to compliance with conditions set forth in the SFA.
Where the common stock are subscribed or purchased under Section 275 of the SFA by a relevant person which is:
| (a) | a corporation (which is not an accredited investor (as defined in Section 4A of the SFA)) the sole business of which is to hold investments and the entire share capital of which is owned by one or more individuals, each of whom is an accredited investor; or |
| (b) | a trust (where the trustee is not an accredited investor) whose sole purpose is to hold investments and each beneficiary of the trust is an individual who is an accredited investor, shares, debentures and units of shares and debentures of that corporation or the beneficiaries’ rights and interest (howsoever described) in that trust shall not be transferred within six months after that corporation or that trust has acquired the common shares pursuant to an offer made under Section 275 of the SFA except: |
| (i) | to an institutional investor (for corporations, under Section 274 of the SFA) or to a relevant person defined in Section 275(2) of the SFA, or to any person pursuant to an offer that is made on terms that such shares, debentures and units of shares and debentures of that corporation or such rights and interest in that trust are acquired at a consideration of not less than S$200,000 (or its equivalent in a foreign currency) for each transaction, whether such amount is to be paid for in cash or by exchange of securities or other assets, and further for corporations, in accordance with the conditions specified in Section 275 of the SFA; |
| (ii) | where no consideration is or will be given for the transfer; or |
| (iii) | where the transfer is by operation of law. |
Switzerland
The common stock may not be publicly offered in Switzerland and will not be listed on the SIX Swiss Exchange (the “SIX”) or on any other stock exchange or regulated trading facility in Switzerland. This document has been prepared without regard to the disclosure standards for issuance prospectuses under art. 652a or art. 1156 of the Swiss Code of Obligations or the disclosure standards for listing prospectuses under art. 27 ff. of the SIX Listing Rules or the listing rules of any other stock exchange or regulated trading facility in Switzerland. Neither this document nor any other offering or marketing material relating to the common shares or the offering may be publicly distributed or otherwise made publicly available in Switzerland.
Neither this document nor any other offering or marketing material relating to the offering, or the common stock have been or will be filed with or approved by any Swiss regulatory authority. In particular, this document will not be filed with, and the offer of common stock will not be supervised by, the Swiss Financial Market Supervisory Authority FINMA, and the offer of common shares has not been and will not be authorized under the Swiss Federal Act on Collective Investment Schemes (“CISA”). Accordingly, no public distribution, offering or advertising, as defined in CISA, its implementing ordinances and notices, and no distribution to any non-qualified investor, as defined in CISA, its implementing ordinances and notices, shall be undertaken in or from Switzerland, and the investor
190
Table of Contents
protection afforded to acquirers of interests in collective investment schemes under CISA does not extend to acquirers of common stock.
United Arab Emirates
This offering has not been approved or licensed by the Central Bank of the United Arab Emirates (the “UAE”), Securities and Commodities Authority of the UAE and/or any other relevant licensing authority in the UAE including any licensing authority incorporated under the laws and regulations of any of the free zones established and operating in the territory of the UAE, in particular the Dubai Financial Services Authority (“DFSA”), a regulatory authority of the Dubai International Financial Centre (“DIFC”). The offering does not constitute a public offer of securities in the UAE, DIFC and/or any other free zone in accordance with the Commercial Companies Law, Federal Law No 8 of 1984 (as amended), DFSA Offered Securities Rules and Nasdaq Dubai Listing Rules, accordingly, or otherwise. The common shares may not be offered to the public in the UAE and/or any of the free zones.
The common shares may be offered and issued only to a limited number of investors in the UAE or any of its free zones who qualify as sophisticated investors under the relevant laws and regulations of the UAE or the free zone concerned.
France
This prospectus (including any amendment, supplement or replacement thereto) is not being distributed in the context of a public offering in France within the meaning of Article L. 411-1 of the French Monetary and Financial Code (Code monétaire et financier).
This prospectus has not been and will not be submitted to the French Autorité des marchés financiers (the “AMF”) for approval in France and accordingly may not and will not be distributed to the public in France.
Pursuant to Article 211-3 of the AMF General Regulation, French residents are hereby informed that:
| 1. | the transaction does not require a prospectus to be submitted for approval to the AMF; |
| 2. | persons or entities referred to in Point 2°, Section II of Article L. 411-2 of the Monetary and Financial Code may take part in the transaction solely for their own account, as provided in Articles D. 411-1, D. 734-1, D. 744-1, D. 754-1 and D. 764-1 of the Monetary and Financial Code; and |
| 3. | the financial instruments thus acquired cannot be distributed directly or indirectly to the public otherwise than in accordance with Articles L. 411-1, L. 411-2, L. 412-1 and L. 621-8 to L. 621-8-3 of the Monetary and Financial Code. |
This prospectus is not to be further distributed or reproduced (in whole or in part) in France by the recipients of this prospectus. This prospectus has been distributed on the understanding that such recipients will only participate in the issue or sale of our common stock for their own account and undertake not to transfer, directly or indirectly, our common stock to the public in France, other than in compliance with all applicable laws and regulations and in particular with Articles L. 411-1 and L. 411-2 of the French Monetary and Financial Code.
191
Table of Contents
The validity of the shares of common stock offered by this prospectus will be passed upon for us by our counsel, Dentons US LLP. Certain legal matters will be passed upon for the underwriters by Latham & Watkins LLP. Members of Dentons US LLP own an interest representing more than $50,000 of our common stock.
The consolidated financial statements of Electrocore, LLC, subsidiaries and affiliate as of December 31, 2016 and 2017, and for each of the years in the two-year period ended December 31, 2017, have been included herein and in the registration statement in reliance upon the report of KPMG LLP, independent registered public accounting firm, appearing elsewhere herein, and upon the authority of said firm as experts in accounting and auditing.
WHERE YOU CAN FIND MORE INFORMATION
We have filed with the SEC a registration statement on Form S-1 under the Securities Act with respect to the shares of common stock offered hereby. This prospectus, which constitutes a part of the registration statement, does not contain all of the information set forth in the registration statement or the exhibits filed therewith. For further information about us and the common stock offered hereby, reference is made to the registration statement and the exhibits filed therewith. Statements contained in this prospectus regarding the contents of any contract or any other document that is filed as an exhibit to the registration statement are not necessarily complete, and in each instance we refer you to the copy of such contract or other document filed as an exhibit to the registration statement. A copy of the registration statement and the exhibits filed therewith may be inspected without charge at the public reference room maintained by the SEC, located at 100 F Street, NE, Washington, DC 20549, and copies of all or any part of the registration statement may be obtained from that office. Please call the SEC at 1-800-SEC-0330 for further information about the public reference room. The SEC also maintains a website that contains reports, proxy and information statements and other information regarding registrants that file electronically with the SEC. The address of the website is www.sec.gov.
We currently do not file periodic reports with the SEC. Upon the closing of our initial public offering, we will be required to file periodic reports, proxy statements and other information with the SEC pursuant to the Exchange Act. These periodic reports, proxy statements and other information will be available for inspection and copying at the SEC’s public reference facilities and the website of the SEC referred to above.
We also maintain a website at www.electrocore.com. Upon completion of this offering, you may access these materials at our website free of charge as soon as reasonably practicable after they are electronically filed with, or furnished to, the SEC. Information contained on our website is not a part of this prospectus and the inclusion of our website address in this prospectus is an inactive textual reference only.
192
Table of Contents
ELECTROCORE, LLC, SUBSIDIARIES AND AFFILIATE
Index to Consolidated Financial Statements
F-1
Table of Contents
Report of Independent Registered Public Accounting Firm
The Board of Directors
Electrocore, LLC:
We have audited the accompanying consolidated balance sheet of Electrocore, LLC, its subsidiaries and its affiliate, as of December 31, 2016, and the related consolidated statements of operations, comprehensive loss, changes in members’ equity (deficit), and cash flows for the year then ended. These consolidated financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on these consolidated financial statements based on our audit.
We conducted our audit in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. An audit includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements. An audit also includes assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audit provides a reasonable basis for our opinion.
In our opinion, the consolidated financial statements referred to above present fairly, in all material respects, the financial position of Electrocore LLC, its subsidiaries and its affiliate as of December 31, 2016, and the results of their operations and their cash flows for the year then ended, in conformity with U.S. generally accepted accounting principles.
KPMG LLP
Short Hills, New Jersey
February 13, 2018
F-2
Table of Contents
ELECTROCORE, LLC, SUBSIDIARIES AND AFFILIATE
December 31, 2016
| Assets |
||||
| Current assets: |
||||
| Cash and cash equivalents |
$ | 416,336 | ||
| Accounts receivable, net |
24,710 | |||
| Inventories |
48,471 | |||
| Prepaid expenses and other current assets |
16,422 | |||
|
|
|
|||
| Total current assets |
505,939 | |||
| Property and equipment – net |
48,426 | |||
| Security deposits |
67,651 | |||
|
|
|
|||
| Total assets |
$ | 622,016 | ||
|
|
|
|||
| Liabilities and Members’ Equity (Deficit) |
||||
| Current liabilities: |
||||
| Accounts payable and accrued expenses |
$ | 3,296,539 | ||
| Warrant liability |
480,636 | |||
| Derivative instrument related to convertible bridge notes |
358,146 | |||
|
|
|
|||
| Total current liabilities |
4,135,321 | |||
| Noncurrent liabilities: |
||||
| Convertible bridge notes, net of unamortized debt discount and issuance costs of $1,955,137 |
3,665,993 | |||
| Deferred rent |
355,724 | |||
|
|
|
|||
| Total liabilities |
8,157,038 | |||
|
|
|
|||
| Commitments and contingencies (Note 15) |
||||
| Members’ equity (deficit): |
||||
| Series A Preferred Units, 70,918,506 Units authorized, 70,918,506 Units issued and outstanding |
53,518,463 | |||
| Common Units, 150,000,000 Units authorized; 90,711,018 Units issued and outstanding |
30,912,091 | |||
| Additional paid-in capital |
8,126,416 | |||
| Accumulated deficit |
(100,706,419 | ) | ||
| Accumulated other comprehensive income |
214,006 | |||
|
|
|
|||
| Total equity (deficit) attributable to Electrocore, LLC, subsidiaries and affiliate |
(7,935,443 | ) | ||
| Noncontrolling interest |
400,421 | |||
|
|
|
|||
| Total members’ equity (deficit) |
(7,535,022 | ) | ||
|
|
|
|||
| Total liabilities and members’ equity (deficit) |
$ | 622,016 | ||
|
|
|
|||
See accompanying notes to consolidated financial statements.
F-3
Table of Contents
ELECTROCORE, LLC, SUBSIDIARIES AND AFFILIATE
Consolidated Statement of Operations
Year ended December 31, 2016
| Net sales |
$ | 254,138 | ||
| Cost of goods sold |
123,731 | |||
|
|
|
|||
| Gross profit |
130,407 | |||
| Operating expenses: |
||||
| Research and development |
7,971,342 | |||
| Selling, general and administrative |
7,169,305 | |||
|
|
|
|||
| Total operating expenses |
15,140,647 | |||
|
|
|
|||
| Loss from operations |
(15,010,240 | ) | ||
| Amortization of debt discount and issuance costs |
536,893 | |||
| Interest expense |
234,352 | |||
|
|
|
|||
| Net loss |
(15,781,485 | ) | ||
| Less: Net loss attributable to noncontrolling interest |
(44,146 | ) | ||
|
|
|
|||
| Net loss attributable to Electrocore, LLC, subsidiaries and affiliate |
$ | (15,737,339 | ) | |
|
|
|
|||
| Pro forma net loss per Unit – Basic and Diluted (unaudited) (Note 8) |
$ | (0.10 | ) | |
|
|
|
|||
| Pro forma weighted average number of Common Units used to calculate net loss per Unit – Basic and Diluted (unaudited) (Note 8) |
150,566,206 | |||
|
|
|
See accompanying notes to consolidated financial statements.
F-4
Table of Contents
ELECTROCORE, LLC, SUBSIDIARIES AND AFFILIATE
Consolidated Statement of Comprehensive Loss
Year ended December 31, 2016
| Net loss |
$ | (15,781,485 | ) | |
| Other comprehensive income: |
||||
| Foreign currency translation adjustment |
8,742 | |||
|
|
|
|||
| Comprehensive loss |
(15,772,743 | ) | ||
| Less: Net comprehensive loss attributable to noncontrolling interest |
(59,067 | ) | ||
|
|
|
|||
| Net comprehensive loss attributable to Electrocore, LLC, subsidiaries and affiliate |
$ | (15,713,676 | ) | |
|
|
|
See accompanying notes to consolidated financial statements.
F-5
Table of Contents
ELECTROCORE, LLC, SUBSIDIARIES AND AFFILIATE
Consolidated Statement of Changes in Members’ Equity (Deficit)
Year ended December 31, 2016
| Series
A Preferred Units |
Common Units |
Additional paid-in capital |
Treasury units |
Accumulated deficit |
Accumulated other comprehensive income |
Equity
(deficit) attributable to Electrocore, LLC, subsidiaries and affiliate |
Noncontrolling interest |
Total members’ equity (deficit) |
||||||||||||||||||||||||||||||||||||
| Units | Amount | Units | Amount | |||||||||||||||||||||||||||||||||||||||||
| Balances as of January 1, 2016 |
63,327,023 | $ | 47,325,765 | 80,029,864 | $ | 30,912,091 | $ | 6,764,497 | $ | (82,658 | ) | $ | (84,969,080 | ) | $ | 190,343 | $ | 140,958 | $ | 399,518 | $ | 540,476 | ||||||||||||||||||||||
| Net loss |
— | — | — | — | — | — | (15,737,339 | ) | — | (15,737,339 | ) | (44,146 | ) | (15,781,485 | ) | |||||||||||||||||||||||||||||
| Other comprehensive income |
— | — | — | — | — | — | — | 23,663 | 23,663 | (14,921 | ) | 8,742 | ||||||||||||||||||||||||||||||||
| Issuance of Series A Preferred Units, net |
4,266,741 | 3,366,667 | — | — | — | — | — | — | 3,366,667 | — | 3,366,667 | |||||||||||||||||||||||||||||||||
| Conversion of term loan, including accrued interest to Series A Preferred Units, net |
1,529,335 | 1,299,935 | — | — | — | — | — | — | 1,299,935 | — | 1,299,935 | |||||||||||||||||||||||||||||||||
| Conversion of convertible bridge notes, including accrued interest to Series A Preferred Units |
1,795,407 | 1,526,096 | — | — | — | — | — | — | 1,526,096 | — | 1,526,096 | |||||||||||||||||||||||||||||||||
| Noncontrolling interest contributions |
— | — | — | — | — | — | — | — | — | 59,970 | 59,970 | |||||||||||||||||||||||||||||||||
| Unit-based compensation |
— | — | — | — | 142,583 | — | — | — | 142,583 | — | 142,583 | |||||||||||||||||||||||||||||||||
| Cancellation of Treasury Units |
— | — | — | — | (82,658 | ) | 82,658 | — | — | — | — | — | ||||||||||||||||||||||||||||||||
| Common Units issued in connection with convertible bridge notes, net |
— | — | 10,681,154 | — | 1,301,994 | — | — | — | 1,301,994 | — | 1,301,994 | |||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
| Balances as of December 31, 2016 |
70,918,506 | $ | 53,518,463 | 90,711,018 | $ | 30,912,091 | $ | 8,126,416 | $ | — | $ | (100,706,419 | ) | $ | 214,006 | $ | (7,935,443 | ) | $ | 400,421 | $ | (7,535,022 | ) | |||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
See accompanying notes to consolidated financial statements.
F-6
Table of Contents
ELECTROCORE, LLC, SUBSIDIARIES AND AFFILIATE
Consolidated Statement of Cash Flows
Year ended December 31, 2016
| Cash flows from operating activities: |
||||
| Net loss |
$ | (15,781,485 | ) | |
| Adjustments to reconcile net loss to net cash used in operating activities: |
||||
| Amortization of debt issuance costs and debt discount |
536,893 | |||
| Unit-based compensation |
142,583 | |||
| Depreciation and amortization |
53,425 | |||
| Loss on disposal of property and equipment |
2,474 | |||
| Changes in operating assets and liabilities: |
||||
| Accounts receivable, net |
75,113 | |||
| Inventories |
1,006 | |||
| Prepaid expenses and other current assets |
67,331 | |||
| Accounts payable and accrued expenses |
1,673,414 | |||
| Deferred rent |
3,481 | |||
|
|
|
|||
| Net cash used in operating activates |
(13,225,765 | ) | ||
|
|
|
|||
| Cash flows from financing activities: |
||||
| Proceeds from issuance of Series A Preferred Units |
3,366,667 | |||
| Proceeds from issuance of convertible bridge notes |
7,121,130 | |||
| Repayment of term loan |
(1,250,000 | ) | ||
| Other proceeds, net |
32,515 | |||
|
|
|
|||
| Net cash provided by financing activities |
9,273,312 | |||
|
|
|
|||
| Effect of changes in exchange rates on cash and cash equivalents |
43,301 | |||
| Net decrease in cash and cash equivalents |
(3,909,152 | ) | ||
| Cash and cash equivalents – beginning of year |
4,325,488 | |||
|
|
|
|||
| Cash and cash equivalents – end of year |
$ | 416,336 | ||
|
|
|
|||
| Supplemental schedule of noncash financing activity: |
||||
| Conversion of term loan, including accrued interest, to Series A Preferred Units, net |
$ | 1,299,935 | ||
| Conversion of convertible bridge notes, including accrued interest, to Series A Preferred Units |
1,526,096 | |||
| Common Units issued in connection with convertible bridge notes |
1,301,994 | |||
| Warrants issued in connection with convertible bridge notes |
480,636 | |||
| Debt issuance costs included in accounts payable |
250,215 | |||
| Cash paid during the year for: |
||||
| Interest |
$ | 43,209 |
See accompanying notes to consolidated financial statements.
F-7
Table of Contents
ELECTROCORE, LLC, SUBSIDIARIES AND AFFILIATE
Notes to Consolidated Financial Statements
December 31, 2016
| (1) | Business and Organization |
Electrocore, LLC (electroCore) is a bioelectronic medicine company, engaged in developing a range of patient-administered non-invasive Vagus Nerve Stimulation (nVNS) therapies initially focused on the treatment of multiple conditions in neurology, rheumatology and other fields. electroCore was founded in 2005 and its focus currently is on primary headache (migraine and cluster headache), with trials continuing in other neurological and inflammatory disorders.
electroCore, headquartered in New Jersey, has wholly owned subsidiaries as follows: electroCore Bermuda, Ltd., electroCore Germany GmbH, and electroCore UK Ltd. In addition, an affiliate, electroCore (Aust) Pty Limited, is subject to electroCore’s control on bases other than voting interests and is a variable interest entity (VIE), for which electroCore is the primary beneficiary.
electroCore, its wholly owned subsidiaries and electroCore (Aust) Pty Limited are collectively referred to as the Company.
In Europe, the Company has received CE Marks for its noninvasive neuro-stimulation therapy (gammaCore®) to treat primary headache, bronchoconstriction, epilepsy, gastric motility disorders, and depression and anxiety.
In April 2017, U.S. Food and Drug Administration (FDA) released the use of gammaCore®, a non-invasive vagus nerve stimulator therapy, for the acute treatment of pain associated with episodic cluster headache in adult patients. gammaCore® transmits a mild electrical stimulation to the vagus nerve through the skin, resulting in a reduction of pain, besides other benefits. This was the first FDA product release for the Company in the U.S.
In January 2018, the FDA released the use of gammaCore® for the treatment of pain associated with migraine headache in adult patients.
| (2) | Summary of Significant Accounting Policies |
(a) Principles of Consolidation
The accompanying consolidated financial statements include the accounts of electroCore and its wholly owned subsidiaries. electroCore (Aust) Pty Limited, a VIE for which electroCore is the primary beneficiary, is also consolidated with the non-controlled equity presented as non-controlling interest. All intercompany balances and transactions have been eliminated in consolidation.
(b) Use of Estimates
The preparation of financial statements in conformity with U.S. generally accepted accounting principles requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the consolidated financial statements and the reported amounts of revenues and expenses during the reporting period. Actual results could differ from those estimates. Significant items subject to such estimates and assumptions include the useful lives of fixed assets; allowances for doubtful accounts and sales returns; valuation of inventory, property and equipment, warrants and derivative instruments, Unit-based compensation, and contingencies.
F-8
Table of Contents
ELECTROCORE, LLC, SUBSIDIARIES AND AFFILIATE
Notes to Consolidated Financial Statements—(Continued)
December 31, 2016
(c) Cash and Cash Equivalents
The Company considers all highly liquid investments with a maturity of three months or less when purchased to be cash equivalents. The Company maintains its U.S. operating cash balances in financial institutions which are insured by the Federal Deposit Insurance Corporation (FDIC) up to $250,000 each. At times, such balances may be in excess of the FDIC insurance limit.
(d) Accounts Receivable
Accounts receivable are recorded at the invoiced amount and do not bear interest. The Company maintains an allowance for doubtful accounts for estimated losses inherent in its accounts receivable portfolio. Management considers an account receivable to be past due when it is not settled under its stated terms. In establishing the required allowance, management considers historical losses adjusted to take into account current market conditions and customers’ financial condition, the amount of receivables in dispute, and the current receivables aging and current payment patterns. Account balances are charged off against the allowance after all means of collection have been exhausted and the potential for recovery is considered remote. The Company does not have any off balance sheet credit exposure related to its customers.
The Company controls its exposure to credit risk through credit analysis and approvals, credit limits, and monitoring procedures. Collateral is generally not required for the Company’s accounts receivables. Management believes the credit risk is limited.
(e) Inventories
Inventories are stated at the lower of cost or market. Cost is determined using the weighted average method.
(f) Property and Equipment
Property and equipment are stated at cost. Depreciation and amortization is computed by the straight line method based on the estimated useful lives of the respective assets, as discussed below. Leasehold improvements are amortized over the lesser of the lease terms or the estimated useful lives of the assets. Amounts expended for maintenance and repairs are charged to expense as incurred, and expenditures for major renewals and improvements are capitalized. Upon disposition of property and equipment, the related cost and accumulated depreciation and amortization are removed from the accounts, and any gain or loss is reflected in the accompanying Consolidated Statement of Operations.
Depreciation is computed using the following estimated useful lives:
| Machinery and equipment |
3 – 15 years | |||
| Furniture and fixtures |
5 – 10 years | |||
| Computer equipment |
5 years |
(g) Impairment of Long-Lived Assets
Long lived assets, such as property, plant, and equipment, are reviewed for impairment whenever events or changes in circumstances indicate that the carrying amount of an asset may not be recoverable. If circumstances require a long lived asset or asset group be tested for possible impairment, the Company
F-9
Table of Contents
ELECTROCORE, LLC, SUBSIDIARIES AND AFFILIATE
Notes to Consolidated Financial Statements—(Continued)
December 31, 2016
first compares undiscounted cash flows expected to be generated by that asset or asset group to its carrying amount. If the carrying amount of the long lived asset or asset group is not recoverable on an undiscounted cash flow basis, an impairment is recognized to the extent that the carrying amount exceeds its fair value. Fair value is determined through various valuation techniques including discounted cash flow models, quoted market values and third party independent appraisals, as considered necessary.
(h) Members’ Equity (Deficit)
The Company’s Units have no par value. Each member’s liability is limited to the respective members’ equity. Additional paid-in capital represents recognition of Unit-based compensation, warrants classified as equity instruments, and the fair value of Common Units issued in connection with certain Convertible Bridge Notes. The Company records cost of repurchasing member Units as Treasury Units.
(i) Revenue Recognition
The Company recognizes revenue when products are shipped and the customer takes ownership and assumes risk of loss, collection of the relevant receivable is probable, persuasive evidence of an arrangement exists and the sales price is fixed or determinable.
(j) Research and Development
Research and development costs are expensed as incurred.
(k) Unit-based Compensation
The Company measures Unit-based compensation at grant-date fair value and recognizes employee compensation expense on a straight-line basis over the vesting period of the award.
Measurement of Unit-based payment transactions with non-employees is based on the fair value of whichever is more reliably measurable: (a) the goods or services received; or (b) the equity instruments issued. The fair value of the Unit-based payment transaction is determined at the earlier of performance commitment date or performance completion date.
Determining the appropriate fair value of Unit-based awards requires the input of subjective assumptions, including the fair value of the Company’s Units, the expected life of the Units, and expected volatility. The Company used the Black-Scholes option pricing model to value its Unit-based awards. The assumptions used in calculating the fair value of Unit-based awards represent management’s best estimates and involve inherent uncertainties and the application of management’s judgment. As a result, if factors change and management uses different assumptions, Unit-based compensation expense could be materially different for future awards.
The expected life of the Units was estimated using the “simplified method,” as the Company has no historical information regarding the expected life of the Units and employment duration for its Unit grants. The simplified method is based on the average of the vesting tranches and the contractual life of each grant. For volatility, the Company uses comparable public companies as a basis for its expected volatility to calculate the fair value of Unit grants. The risk-free interest rate is based on U.S. Treasury notes with a term approximating the expected life of the Unit.
The Company accounts for forfeitures of Unit-based awards as they occur.
F-10
Table of Contents
ELECTROCORE, LLC, SUBSIDIARIES AND AFFILIATE
Notes to Consolidated Financial Statements—(Continued)
December 31, 2016
(l) Warrants and Other Derivative Instruments
In connection with the issuance debt or equity instruments, the Company may issue warrants to purchase equity interests. In certain circumstances, these warrants may be classified as liabilities, rather than as equity. Additionally, the debt or equity instruments may contain embedded derivative instruments, such as variable conversion options, which may be required to be evaluated under the provisions of Financial Accounting Standards Board (FASB) Accounting Standards Codification (ASC) Topic 815, Derivatives and Hedging (ASC Topic 815), bifurcated from the host instrument and accounted for separately as a derivative instrument liability.
In 2016, related to the issuance of certain convertible Bridge Notes, the Company issued warrants and recorded them as liabilities as the exercise price for such warrants was undetermined at the time of their issuance. In addition, the Company also recognized an embedded derivative related to the conversion option of the Bridge Notes. The warrants were valued using the probability weighted expected return method and option pricing models. The embedded derivative instrument was recorded at fair value using an alternative discounted cash flow method. Key assumptions used in the valuation model were based on the terms and conditions of the warrants and the embedded derivative. These warrants and derivative instruments are remeasured at each balance sheet date (or upon exercise of warrant) with changes in fair value recorded as amortization of debt discount and issuance costs in the Consolidated Statement of Operations.
(m) Foreign Currency Translation and Transactions
Operations in non-U.S. entities are recorded in the functional currency of each entity. For financial reporting purposes, the functional currency of an entity is determined by a review of the source of an entity’s most predominant cash flows. The results of operations for non-U.S. dollar functional currency entities are translated from functional currencies into U.S. dollars using the average currency rate during each month, which approximates the results that would be obtained using actual currency rates on the dates of individual transactions. Assets and liabilities are translated using currency rates at the end of the period. Adjustments resulting from translating the financial statements of the foreign entities into the U.S. dollar are excluded from the determination of net loss and are recorded as a component of other comprehensive loss. Foreign currency transaction gains and losses related to assets and liabilities that are denominated in a currency other than the functional currency are reported in the Consolidated Statement of Operations in the period they occur.
(n) Income Taxes
The Company is a limited liability company, which is treated as a partnership for Federal and state income tax purposes. Accordingly, the Company is not subject to income taxes. No provision has been made for Federal and state income taxes since these taxes are the personal responsibility of the Members.
(o) Net Comprehensive Loss
Net comprehensive loss consists of net loss and foreign exchange translation adjustments and is presented in the Consolidated Statement of Comprehensive Loss.
(p) Fair Value of Financial Instruments
The Company follows the guidance contained in ASC Topic 820, Fair Value Measurement. At December 31, 2016 the carrying amounts of the Company’s financial instruments, such as cash and cash
F-11
Table of Contents
ELECTROCORE, LLC, SUBSIDIARIES AND AFFILIATE
Notes to Consolidated Financial Statements—(Continued)
December 31, 2016
equivalents, accounts receivable, accounts payable, and accrued expenses approximate their fair values mainly due to the short period to maturity.
The Company utilizes valuation techniques that maximize the use of observable inputs and minimize the use of unobservable inputs to the extent possible. The Company determines fair value based on assumptions that market participants would use in pricing an asset or liability in the principal or most advantageous market.
(q) Segment Information
The Company operates in one reportable segment within the United States, Europe and Australia. Management uses one measurement of profitability and does not segregate its business for internal reporting, making operating decisions, and assessing financial performance. Net sales within the United States and outside the United States were approximately $10,000 and $244,000, respectively, for the year ended December 31, 2016. Sales to a UK and German customer accounted for 57% and 19% of total sales, respectively. All long-lived assets are maintained in the United States.
(r) Recent Accounting Pronouncements
In August 2014, the FASB issued ASU No. 2014-15 regarding ASC Topic No. 205, Presentation of Financial Statements – Going Concern. The standard requires all companies to evaluate if conditions or events raise substantial doubt about an entity’s ability to continue as a going concern and requires different disclosure of items that raise substantial doubt that are, or are not, alleviated as a result of consideration of management’s plans. The new guidance is effective for annual periods ending after December 15, 2016. The Company adopted ASU No. 2014-15 during the year ended December 31, 2016. Note 3 – Significant Risks and Uncertainties incorporates the disclosure requirements from the adoption of ASU 2014-15.
In May 2014, the FASB issued Revenue from Contracts with Customers, Topic 606 (Accounting Standards Update No. 2014-09) (ASU 2014-09), which provides a framework for the recognition of revenue, with the objective that recognized revenues properly reflect amounts an entity is entitled to receive in exchange for goods and services. This guidance will be effective for interim and annual reporting periods beginning after December 15, 2017. The Company is in the process of evaluating the new standard and assessing the impact, if any, ASU 2014-09 will have on the Company’s consolidated financial statements.
In February 2016, the FASB issued ASU No. 2016-02, Leases (Topic 842), which requires lessees to recognize most leases on the balance sheet. The provisions of this guidance are effective for annual periods beginning after December 15, 2018, and interim periods within those years, with early adoption permitted. The Company is assessing ASU No. 2016-02’s impact and will adopt it when effective.
In March 2016, the FASB issued ASU 2016-09, Improvements to Employee Share-Based Payment, which is intended to simplify several aspects of the accounting for share-based payment transactions, including the income tax consequences, classification of awards as either equity or liabilities, the estimation of forfeitures, shares withheld for taxes and classification of shares withheld for taxes on the statement of cash flows. This guidance will be effective for interim and annual reporting periods beginning after December 15, 2016. The Company is assessing ASU No. 2016-09’s impact and will adopt it when effective.
F-12
Table of Contents
ELECTROCORE, LLC, SUBSIDIARIES AND AFFILIATE
Notes to Consolidated Financial Statements—(Continued)
December 31, 2016
In August 2016, the FASB issued ASU No. 2016-15, Statement of Cash Flows: Classification of Certain Cash Receipts and Cash Payments (Topic 230). This ASU will make eight targeted changes to how cash receipts and cash payments are presented and classified in the statement of cash flows. The ASU will be effective for fiscal years beginning after December 15, 2017. This standard will require adoption on a retrospective basis unless it is impracticable to apply, in which case it would be required to apply the amendments prospectively as of the earliest date practicable. The Company is assessing ASU No. 2016-15’s impact and will adopt it when effective.
| (3) | Significant Risks and Uncertainties |
The Company’s budgeted cash requirements in 2017 and beyond include expenses related to continuing development and clinical evaluation of its product and therapies, as well as preparing for related commercialization of the product. Based on the Company’s available cash resources and cash flow projections as of the date the consolidated financial statements were available for issuance, it believes it has sufficient funds to continue its operations and research and development programs at least through February, 2019. Until the Company can generate significant cash from its operations, the Company expects to continue to fund its operations with its available financial resources. These financial resources may not be adequate to sustain its operations and the Company will be required to finance future cash needs through the sale of additional equity or debt securities. However, the Company cannot be certain that additional financing will be available when needed or that, if available, financing will be obtained on terms favorable to the Company or its Members. The capital markets have experienced volatility in recent years, which has resulted in uncertainties with respect to availability of capital and hence the timing to meet an entity’s liquidity needs. Having insufficient funds may require the Company to delay, scale-back or eliminate some or all of its programs or renegotiate less favorable terms than it would otherwise choose. Failure to obtain adequate financing also may adversely affect its ability to operate as a going concern.
In addition to the U.S. Food and Drug Administration (FDA) release received by the Company for two indications (see Note 1), the Company is seeking approvals and clearances by the FDA for additional indications. In connection therewith, the Company will incur additional time and costs and will require additional funding to obtain such approvals and clearances. The additional time, costs, and funding is expected to be substantial.
The Company is highly dependent upon the technical and management skills of several of its officers.
The Company’s potential growth may cause a significant strain on its management, operational, and financial resources. Its ability to manage its growth effectively will require it to continue to implement and improve its operational and financial systems. The Company’s success also depends in large part on a limited number of current key technical, marketing, and sales employees and on the Company’s ability to continue to attract and retain additional highly talented personnel.
The Company has foreign currency exchange risks related to revenue and operating expenses in currencies other than the local currencies in which they operate. The Company is exposed to currency risk from the potential changes in functional currency values of their foreign currency denominated assets, liabilities, and cash flows.
F-13
Table of Contents
ELECTROCORE, LLC, SUBSIDIARIES AND AFFILIATE
Notes to Consolidated Financial Statements—(Continued)
December 31, 2016
| (4) | Fair Value Measurements |
Fair value is defined as the exchange price that would be received for an asset or paid to transfer a liability (an exit price) in the principal or most advantageous market for the asset or liability in an orderly transaction between market participants on the measurement date. Valuation techniques used to measure fair value are performed in a manner to maximize the use of observable inputs and minimize the use of unobservable inputs. ASC Topic 820, Fair Value Measurement, provides the following fair value hierarchy:
| • | Level 1 Inputs: Unadjusted quoted prices in active markets for identical assets or liabilities accessible to the reporting entity at the measurement date. |
| • | Level 2 Inputs: Other than quoted prices included in Level 1 inputs that are observable for the asset or liability, either directly or indirectly, for substantially the full term of the asset or liability. |
| • | Level 3 Inputs: Unobservable inputs for the asset or liability used to measure fair value to the extent that observable inputs are not available, thereby allowing for situations in which there is little, if any, market activity for the asset or liability at measurement date. |
During the year ended December 31, 2016, the Company has not changed the manner in which it values assets and liabilities that are measured at fair value using Level 3 inputs. The Company recognizes transfers between levels of the fair value hierarchy as of the end of the reporting period. There were no transfers within the hierarchy during the year ended December 31, 2016.
A summary of the assets and liabilities carried at fair value in accordance with the hierarchy defined above is as follows:
| Fair Value Hierarchy | ||||||||||||||||
| Carrying Value |
Quoted Prices in active markets for identical instruments (Level 1) |
Significant other observable inputs (Level 2) |
Significant unobservable inputs (Level 3) |
|||||||||||||
| Assets |
||||||||||||||||
| Cash and cash equivalents |
$ | 416,336 | $ | 416,336 | $ | — | $ | — | ||||||||
| Liabilities |
||||||||||||||||
| Warrant liability |
$ | 480,636 | $ | — | $ | — | $ | 480,636 | ||||||||
| Derivative instrument related to convertible Bridge Notes |
$ | 358,146 | $ | — | $ | — | $ | 358,146 | ||||||||
Cash and cash equivalents of $416,336 of December 31, 2016 consisted of cash in bank checking and savings accounts and are classified within Level 1 of the fair value hierarchy because they are valued using quoted market prices in active markets.
The warrant liability was recorded at fair value determined by using the probability weighted expected return method and option pricing models. This method of valuation involves using inputs such as the fair value of the Company’s common units, unit price volatility, the contractual term of the warrant, risk free
F-14
Table of Contents
ELECTROCORE, LLC, SUBSIDIARIES AND AFFILIATE
Notes to Consolidated Financial Statements—(Continued)
December 31, 2016
interest rates and dividend yields. Due to the nature of these inputs, the valuation of the warrant liability was considered a Level 3 measurement.
As of December 31, 2016 and at issuance, the estimated fair value of the warrant liability was computed using the following assumptions:
| Stock price volatility |
71.7 | % | ||
| Risk-free interest rates |
1.33 | % | ||
| Annual dividend yield |
0 | % | ||
| Expected life (years) |
2.50 |
The derivative liability related to the convertible bridge notes was recorded at fair value determined by using an alternative discounted cash flow method. This method of valuation involves using inputs such as (1) a 50% required rate of return, (2) 80% probability of a qualified financing round closing prior to the maturity of the convertible Bridge Notes, (3) option’s ability to convert at a 10% discount into the expected next qualified financing round. Due to the nature of these inputs, the valuation of the derivative instrument was considered a Level 3 measurement.
A roll-forward of the recurring fair value measurements of the liabilities categorized with Level 3 inputs are as follows:
| Warrant liability |
Derivative instrument related to convertible bridge notes |
|||||||
| Opening Balance as of January 1, 2016 |
$ | — | $ | — | ||||
| Additions |
480,636 | 358,146 | ||||||
| Settlements |
— | — | ||||||
| Changes in fair value recognized |
— | — | ||||||
|
|
|
|
|
|||||
| Closing Balance as of December 31, 2016 |
$ | 480,636 | $ | 358,146 | ||||
|
|
|
|
|
|||||
| (5) | Inventories |
Inventories as of December 31, 2016 consisted of the following:
| Raw materials |
$ | 15,267 | ||
| Finished goods |
33,204 | |||
|
|
|
|||
| $ | 48,471 | |||
|
|
|
F-15
Table of Contents
ELECTROCORE, LLC, SUBSIDIARIES AND AFFILIATE
Notes to Consolidated Financial Statements—(Continued)
December 31, 2016
| (6) | Property and Equipment – Net |
Property and equipment – net as of December 31, 2016 consisted of the following:
| Machinery and equipment |
$ | 379,614 | ||
| Furniture and fixture |
87,664 | |||
| Computer equipment |
127,856 | |||
|
|
|
|||
| Property, plant and equipment – gross |
595,134 | |||
| Less accumulated depreciation and amortization |
(546,708 | ) | ||
|
|
|
|||
| Property, plant and equipment – net |
$ | 48,426 | ||
|
|
|
Depreciation and amortization expense for the year ended December 31, 2016 was $53,425.
| (7) | Accounts Payable and Accrued Expenses |
Accounts payable and accrued expenses as of December 31, 2016 consisted of the following:
| Accounts payable |
$ | 2,241,117 | ||
| Accrued expenses |
740,832 | |||
| Due to employees |
225,963 | |||
| Accrued interest expense |
88,627 | |||
|
|
|
|||
| $ | 3,296,539 | |||
|
|
|
| (8) | Pro Forma Net Loss Per Unit (Unaudited) |
Unaudited pro forma basic and diluted net loss per unit for the year ended December 31, 2016, gives effect to the assumed automatic conversion of all the outstanding shares of Series A Preferred Units immediately prior to the closing of the Initial Public Offering (IPO). Prior to the consummation of an IPO each unit of Series A Preferred Units will convert into 70,918,506 shares of the Company’s common stock on a conversion ratio of 1:1. For purposes of pro forma basic and diluted net loss per unit, all Series A Preferred Units have been treated as though they have been converted to common stock at the later of the issuance date or January 1, 2016. Unaudited pro forma loss per unit does not consider shares issued in an IPO.
In addition, unaudited pro forma net loss per Unit gives effect to income tax adjustments as if the Company was a taxable entity as of the beginning of the period. Immediately prior to the effectiveness of the Company’s registration statement, the Company will convert into a C-corporation and will be subject to federal and state income taxes.
The Company has reported a net loss for the year ended December 31, 2016. Further, based on the Company’s history of generating operating losses and its anticipation of operating losses continuing in the foreseeable future, the Company has determined that it would not have been more likely than not that the tax benefits from these net operating losses would be realized and a full valuation allowance against all deferred tax assets would be recorded on a pro forma basis. Therefore, for the purposes of the pro forma tax provision, income tax expense is determined to be zero.
F-16
Table of Contents
ELECTROCORE, LLC, SUBSIDIARIES AND AFFILIATE
Notes to Consolidated Financial Statements—(Continued)
December 31, 2016
The Company has excluded all common equivalent shares outstanding for warrants and convertible instruments from the calculation of diluted net loss per share because all such securities are antidilutive.
The following table summarizes the computation of pro forma basic and diluted net loss per unit attributable to common stockholders for the year ended December 31, 2016.
| Numerator – Basic and Diluted |
||||
| Loss from operations before income taxes |
$ | (15,737,339 | ) | |
| Pro forma provisions/(benefit) for income taxes |
— | |||
|
|
|
|||
| Pro forma net loss |
$ | (15,737,339 | ) | |
|
|
|
|||
| Denominator – Basic and Diluted |
||||
| Weighted average pro forma Common Units outstanding |
82,233,294 | |||
| Weighted average pro forma Common Units issued upon conversion of Series A Preferred Units |
68,332,912 | |||
|
|
|
|||
| Pro forma weighted average number of Common Units |
150,566,206 | |||
|
|
|
|||
| Net loss per Unit, Basic and Diluted |
$ | (0.10 | ) | |
|
|
|
| (9) | Members’ Equity |
The Company’s operating agreement, as amended and restated in March 2013, permits issuance of two classes of Units – Series A Preferred Units and Common Units. Each member is entitled to one vote for each Unit held and the Units of all classes and series shall vote together as a single class on all matters (on an as converted to Common Unit basis). In 2017 the Company’s operating agreement was further amended to create an additional class of preferred equity designated as “Series B Preferred Units” and certain changes were made to the terms of the Common and Series A Preferred Units. See Note 17 (a).
The Series A Preferred Units are entitled to a return in an annual non-compounded amount with respect to each outstanding Series A Preferred Unit equal to the product of the Series A Preferred Return Percentage and the Series A Unreturned Capital Value for each Unit, which shall accrue to the extent not paid. The Series A Preferred Return Percentage is 4% and may be reduced to 2% if certain requirements are met as outlined in the amended and restated operating agreement. Additionally, the payment of the Series A Preferred Return is at the sole discretion of the Board of Managers. The Series A Preferred Return in arrears aggregated to $5,338,142 as of December 31, 2016.
The Series A Preferred Units are convertible at the option of the holder, or upon the occurrence of certain events, mandatorily, into a number of Common Units as outlined in the amended and restated operating agreement. At December 31, 2016, each Series A Preferred Unit was convertible into one Common Unit. In addition, in connection with the Company’s Operating Agreement the Company has the ability to reserve a sufficient number of Common Units to enable the conversion of all Series A Preferred Units.
The amended and restated operating agreement contains specific provisions for payments to the Series A Preferred and Common Unit Members for liquidating and non-liquidating distributions. The Series A Preferred Units also have other protective provisions that prohibits the Company from taking certain actions as outlined in the amended and restated operating agreement without the prior written consent of the holders of not less than 55% of the total outstanding Series A Preferred Units.
F-17
Table of Contents
ELECTROCORE, LLC, SUBSIDIARIES AND AFFILIATE
Notes to Consolidated Financial Statements—(Continued)
December 31, 2016
Following the 2017 amendments to the operating agreement, the Series A Preferred Return payable upon a public offering of the Company’s common stock was fixed at $3,629,092 and is payable, at the Company’s election, in cash or shares of the Company’s common stock.
| (10) | Series A Preferred Financing |
On March 28, 2013, the Company entered into a Series A Preferred Unit Purchase Agreement with Core Ventures II, LLC (CV II), Merck Global Health Innovation Fund, LLC and Conure ElectroCore LLC, all related parties. Under the terms of the Purchase Agreement, as amended, through December 31, 2016, the Company raised an aggregate amount of $50,692,432 through the sale of Series A Preferred Units at an initial closing and several required milestone closings, several optional milestone closings, as well as from the exercise of certain warrants, net of related issuance costs, as follows:
| Closing date |
Number of Series A Preferred Units/ warrants |
Price per unit |
Aggregate issuance price |
Fiscal year | ||||||||||||||||||||||||||
| 2013 | 2014 | 2015 | 2016 | |||||||||||||||||||||||||||
| March 2013 |
20,400,669 | Preferred Units | $ | 0.73527 | $ | 15,000,000 | $ | 15,000,000 | ||||||||||||||||||||||
|
|
|
|||||||||||||||||||||||||||||
| Total, initial closing | $ | 15,000,000 | ||||||||||||||||||||||||||||
|
|
|
|||||||||||||||||||||||||||||
| December 2013 |
4,533,482 | Preferred Units | 0.73527 | $ | 3,333,334 | 3,333,334 | ||||||||||||||||||||||||
| April 2014 |
9,066,964 | Preferred Units | 0.73527 | 6,666,666 | 6,666,666 | |||||||||||||||||||||||||
| June 2014 |
6,800,222 | Preferred Units | 0.73527 | 5,000,000 | 5,000,000 | |||||||||||||||||||||||||
|
|
|
|||||||||||||||||||||||||||||
| Total, required | ||||||||||||||||||||||||||||||
| milestone closing | $ | 15,000,000 | ||||||||||||||||||||||||||||
|
|
|
|||||||||||||||||||||||||||||
| September 2014 |
5,882,353 | Preferred Units | 0.85 | $ | 5,000,000 | 5,000,000 | ||||||||||||||||||||||||
| January 2015 |
5,882,353 | Preferred Units | 0.85 | 5,000,000 | 5,000,000 | |||||||||||||||||||||||||
| April 2015 |
5,882,353 | Preferred Units | 0.85 | 5,000,000 | 5,000,000 | |||||||||||||||||||||||||
| November, 2015 |
2,428,312 | Preferred Units | 0.85 | 2,064,065 | 2,064,065 | |||||||||||||||||||||||||
| March, 2016 |
2,000,000 | Preferred Units | 0.85 | 1,700,000 | 1,700,000 | |||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
| Total, optional | ||||||||||||||||||||||||||||||
| milestone closing | $ | 18,764,065 | 18,333,334 | 16,666,666 | 12,064,065 | 1,700,000 | ||||||||||||||||||||||||
|
|
|
|||||||||||||||||||||||||||||
| November, 2015 |
2,266,741 | Exercise of warrants | 0.73527 | 1,666,667 | ||||||||||||||||||||||||||
| March, 2016 |
2,266,741 | Exercise of warrants | 0.73527 | 1,666,667 | ||||||||||||||||||||||||||
| Issuance costs | (953,466 | ) | (300,000 | ) | (151,501 | ) | — | |||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
| Net proceeds | $ | 17,379,868 | 16,366,666 | 13,579,231 | 3,366,667 | |||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
As of December 31, 2016, all warrants issued in connection with the Series A Preferred Units have either been exercised or have expired.
| (11) | Term Loan |
On December 22, 2015, the Company entered into a Loan and Security Agreement (the Bank Agreement) with Pacific Western Bank (Bank) pursuant to which the Company received a term loan of $1,250,000. The Bank Agreement also provided for three additional term loans aggregating $6,250,000, available at various dates through June 2017. In connection with the financing, the Bank received 66,177 warrants to purchase Series A Preferred Units at an exercise price of $0.85 per Unit. The warrants expire on December 22, 2025.
F-18
Table of Contents
ELECTROCORE, LLC, SUBSIDIARIES AND AFFILIATE
Notes to Consolidated Financial Statements—(Continued)
December 31, 2016
One of the conditions related to the Bank Agreement required the Company to receive proceeds of not less than $8,000,000 on or prior to April 30, 2016, from the issuance of Series A Preferred Units. Due to the Company’s failure to comply with such requirement, the Bank delivered a Notice of Default and in May 2016, the Company repaid the $1,250,000 term loan balance in full and the Bank Agreement was terminated.
On December 22, 2015, the Company also entered into a Loan and Security Agreement (CV II Agreement) with CV II pursuant to which the Company received a term loan from CV II of $1,250,000 (CV II term loan). The CV II term loan was subordinated to the term loan received from the Bank. In connection with the financing, CV II received 66,177 warrants to purchase Series A Preferred Units at an exercise price of $0.85 per Unit. The warrants expire on December 22, 2025.
Pursuant to the terms of the CV II Agreement, CV II opted to convert the term loan of $1,250,000 and related accrued interest of $49,935 into the Company’s Series A Preferred Units in 2016, at a per Unit price of $0.85 per Unit.
The fair value of the warrants issued to the Bank and CV II aggregated $59,030. The Company also incurred issuance costs related to the financing of $134,137. The fair value of the warrants and issuance costs attributable to the loan per Bank Agreement aggregating $96,584 were recognized under amortization of debt discount and issuance costs for the year ended December 31, 2016. The fair value of the warrants and issuance costs attributable to the proceeds received from the CV II term loan aggregating $96,583 were recognized as a reduction from the amount allocated to Series A Preferred Units.
Interest on both the loans were payable at a variable annual rate of 7.30% plus LIBOR subject to a minimum of 7.5%.
As of December 31, 2016, 132,354 warrants to purchase Series A Preferred Units, issued in connection with the term loans remained outstanding.
| (12) | Convertible Bridge Notes |
Beginning in June 2016, the Company commenced raising new capital under a Bridge Note and Warrant Purchase Agreement (the Bridge Note). Under the original terms of the Bridge Note, investors were entitled to annual interest at 10%, warrant coverage equal to 20% of the face value of the investment, and the right to convert the face value and accrued interest upon the Company’s next bona fide equity financing round that raised not less than $8 million (exclusive of the Bridge Notes) (Qualified Equity Round) into the equity securities issued in such round at a 10% discount to the purchase price payable for such equity securities in the Qualified Equity Round (the Next Round Price). In addition, the Bridge Notes are also convertible into Series A Preferred Units at $0.85 per Unit, at the option of the investors. In September 2016 the terms of the bridge financing were amended (September 2016 amendment) to provide that subsequent purchasers of Bridge Notes would also receive up to two Common Units for each one dollar of principal amount of Bridge Note purchased. The warrants issued in connection with the Bridge Notes are exercisable for a period of five years and entitle each holder to purchase an amount of securities issued in the Qualified Equity Round equal to 20% of principal amount of the Bridge Notes purchased by each such investor divided by the Next Round Price, with an exercise price equal to the Next Round Price. For Bridge Note closings completed prior to the September 2016 amendment, the
F-19
Table of Contents
ELECTROCORE, LLC, SUBSIDIARIES AND AFFILIATE
Notes to Consolidated Financial Statements—(Continued)
December 31, 2016
warrants are for the purchase of the Company’s Series A Preferred Units (together, Bridge Note Warrants).
In 2016, the Company issued Bridge Note aggregating $7,121,130 (including $5,060,025 purchased by CV II and $1,500,000 purchased by ECNG, LLC (ECNG), an investor affiliated with CV II). In September 2016, ECNG elected to convert $1,500,000 of its holdings in Bridge Notes, and accrued interest of $26,096, into 1,795,407 Series A Preferred Units. The remaining Bridge Notes issued remained outstanding as of December 31, 2016, with a maturity date of one year from the applicable original issuance dates. In connection with the Bridge Note closings, at the time of the Qualified Equity Round, the Company will issue 2,144,337 Bridge Note Warrants.
Since the Bridge Note Warrants entitle the holders to purchase securities in the Qualified Equity Round at the purchase price payable for the related equity securities, the exercise price of the warrants was undetermined at the time of their issuance. Accordingly, the warrants were recorded as liabilities.
Under ASC Topic 815, certain contractual terms that meet the accounting definition of a derivative must be accounted for separately from the financial instrument in which they are embedded. The Company has concluded that the right of the Bridge Note investors to convert the face value and accrued interest to Company’s equity securities constitutes embedded derivatives.
The Company determined the amount attributable to the Common Units issued in 2016 in connection with the Bridge Notes at relative fair value at $1,274,804 and the amounts attributable to Bridge Note Warrants and embedded derivatives related to Qualified Equity Financing at fair values at $480,636 and $358,146 respectively. The fair value for the embedded derivative related to the option to convert to Series A Preferred Units was deemed immaterial.
As of December 31, 2016, the amount related to Common Units, Bridge Note Warrants and the embedded derivatives were recorded as a discount on the Bridge Notes and are being amortized over the maturity term of the respective Bridge Notes. At December 31, 2016, the unamortized discount on the Bridge Notes was $1,758,361.
In connection with the bridge financing, the Company engaged two advisors (the Advisors) to serve as placement agents. The Advisors are entitled to a combined placement agent fee of 10% of the principal amount of the Bridge Notes sold to investors first introduced to the Company by the Advisors, five-year warrants to purchase securities in the Qualified Equity Round at the purchase price payable for the related equity securities (Advisor Warrants), and right to purchase 9% of the number of securities issuable upon the conversion of the Bridge Notes issued to such investors. In addition, one of the Advisors is also entitled to receive one-half of a Common Unit for each one dollar of principal amount of Bridge Notes purchased by investors first introduced to the Company by such Advisor.
During the year ended December 31, 2016, the Advisors sold Bridge Notes for the principal amount of $561,105. With respect to such Bridge Notes and associated Common Units and Bridge Note Warrants, the Company incurred total costs of $133,289 (inclusive of $15,712 representing fair value of 72,142 Advisor Warrants, to be issued by the Company at the time of the Qualified Equity Round); $109,933 of such amount was recognized as a discount on the Bridge Notes and will be amortized over the maturity term of the Bridge Notes. Based on the fair values of the financial instruments issued in connection with the Bridge Notes, the remaining amount was allocated as follows: $9,282 to Common Units and $14,014
F-20
Table of Contents
ELECTROCORE, LLC, SUBSIDIARIES AND AFFILIATE
Notes to Consolidated Financial Statements—(Continued)
December 31, 2016
to Bridge Note Warrants. The amount allocated to Common Units was netted against the related proceeds and the amount related to Bridge Note Warrants was expensed during the year ended December 31, 2016.
The Company uses Level 3 inputs for its valuation methodology for the warrant liability and embedded derivatives. The carrying value of the Company’s Bridge Notes approximated fair value as the interest rate for such notes approximated market rates of interest available to the Company for similar instruments as well as because of their short maturity.
As mentioned in Note 17 (c) below, in 2017, the Bridge Notes were converted to the Company’s newly issued Series B Preferred Units. Accordingly, as permitted by ASC Topic 470-10-45-14, Debt, as of December 31, 2016, the Bridge Notes have been classified as long-term liabilities.
| (13) | Unit-Based Compensation |
In connection with employment and service provider agreements the Company has awarded grantees Units that constitute profits interests for income tax purposes, subject to certain restrictions defined in each Unit forfeiture agreement. The Company maintains a Unit award account for each of the grantees. Generally, the Units vest 25% on the one year anniversary of the employment start date or agreement date and the balance ratably per quarter thereafter over an additional three year period. After the restrictions lapse, the grantees become fully vested in such Units.
The following summarizes activity related to the Company’s unvested Unit awards for the year ended December 31, 2016:
| Number of units |
Weighted average grant date fair value |
|||||||
| Outstanding, beginning of the year |
3,052,914 | $ | 0.06 | |||||
| Granted |
11,251,553 | $ | 0.08 | |||||
| Vested |
(845,449 | ) | $ | 0.05 | ||||
| Forfeited |
(1,934,170 | ) | $ | 0.05 | ||||
|
|
|
|||||||
| Outstanding, end of the year |
11,524,848 | $ | 0.08 | |||||
|
|
|
|||||||
As of December 31, 2016 there were $878,471 of total unrecognized compensation cost related to unvested Unit-based compensation awards respectively, which are expected to be recognized over a weighted average period of four years.
The Company utilizes the Black Scholes option pricing model for estimating the fair value of all Units granted. The fair value of each Unit is estimated on the date of the grant. The fair value is then amortized using graded-vesting over the requisite service period for each separately vesting portion of the award as if the award was, in-substance, multiple awards.
F-21
Table of Contents
ELECTROCORE, LLC, SUBSIDIARIES AND AFFILIATE
Notes to Consolidated Financial Statements—(Continued)
December 31, 2016
The weighted average assumptions for the Units granted during the year ended December 31, 2016 are provided in the following table:
| Valuation assumptions: |
||||
| Expected dividend yield |
0 | % | ||
| Expected volatility |
79.10 | % | ||
| Expected term (years) |
2.01 | |||
| Risk-free interest rate |
0.64 | % |
The risk-free interest rate is the average U.S. Treasury rate with a term that most closely resembles the expected life of the award for the year in which the award was granted. The expected life is the period of time that the awards granted are expected to remain outstanding. The expected life is calculated using a simplified method, as permitted by the accounting standards. Expected volatility is a measure of the amount by which the Unit price has fluctuated or is expected to fluctuate during a period. For volatility, the Company uses comparable public companies as a basis for its expected volatility. The Company does not pay regular dividends on its Units and does not anticipate paying any dividends in the foreseeable future.
For the year ended December 31, 2016, Unit-based compensation expense is reported as a component of selling, general and administrative expense in the Company’s Consolidated Statement of Operations.
| (14) | Variable Interest Entity |
As discussed in note 1, electroCore is the primary beneficiary of electroCore (Aust) Pty Limited. electroCore has contributed certain intellectual property rights, all rights to distribute, market and sell specified products in Australia and New Zealand, and other rights outlined in the shareholders’ deed of electroCore (Aust) Pty Limited in return for 50% of the shares of such entity. In addition, electroCore can also appoint two of the four directors and can exercise significant influence. This along with the fact that electroCore is electroCore (Aust) Pty Limited’s only supplier causes electroCore, for accounting purposes, to be the primary beneficiary of electroCore (Aust) Pty Limited. The activities related to electroCore (Aust) Pty Limited are not material to the consolidated financial statements.
| (15) | Commitments and Contingencies |
(a) Operating Lease
The Company leases office space under operating leases through April 2022. Future minimum lease payments under non-cancelable operating leases (with initial or remaining lease terms in excess of one year) as of December 31, 2016 are as follows:
| Year ending December 31: |
||||
| 2017 |
$ | 540,110 | ||
| 2018 |
552,524 | |||
| 2019 |
564,939 | |||
| 2020 |
577,353 | |||
| 2021 |
545,472 | |||
| 2022 |
195,437 | |||
|
|
|
|||
| $ | 2,975,835 | |||
|
|
|
F-22
Table of Contents
ELECTROCORE, LLC, SUBSIDIARIES AND AFFILIATE
Notes to Consolidated Financial Statements—(Continued)
December 31, 2016
For the year ended December 31, 2016, rental expense related to the leases was $529,271.
(b) Legal Proceedings
The Company may from time to time be involved in various claims and legal actions arising in the ordinary course of its business. In the opinion of management, the ultimate disposition of any of these matters will not have a material adverse effect on the Company’s consolidated financial position, results of operations, or liquidity.
| (16) | Employee Benefit Plan |
The Company has a defined contribution 401(k) profit sharing plan which covers all employees. Employees are eligible upon date of hire. Employee contributions are voluntary and are based on specific percentages of compensation, which may not exceed maximum amounts established by Internal Revenue Code. Employer contributions are discretionary. There were no employer contributions for the year ended December 31, 2016.
| (17) | Subsequent Events |
The Company has evaluated subsequent events from the balance sheet date through February 13, 2018, the date at which the consolidated financial statements were available to be issued, and determined there are no other items to disclose, except as disclosed below and in notes 1, 9 and 12.
(a) Amendment of Operating Agreement
The Company’s Operating Agreement was amended and restated in August 2017 and again in November 2017 in connection with multiple closings under its Series B financing. Pursuant to such amendments, the authorized capital of the Company consists of Common Units, Series A Preferred Units, and Series B Preferred Units. The Series B Preferred Units are convertible at the option of the holder, or in certain circumstances mandatorily, into a number of Common Units as outlined in the amended and restated operating agreement.
Pursuant to such amendments, the total number of Units of all classes and series of Membership Interests which the Company is authorized to issue is as follows: (i) 500,000,000 Common Units; (ii) 71,050,860 Series A Preferred Units; and (iii) 101,812,060 Series B Preferred Units.
In 2017, in exchange for the elimination of a portion of the preference amount of $54,923,430, payable to the holders of the Series A Preferred Units, each holder of the Series A Preferred Units received Common Units based on a fraction where the numerator was the issue price for the Series A Preferred Units held and the denominator was 1.17. Similarly, in 2017, for the elimination of the entire preference amount of $30,912,091 payable to the Common Investors, as defined in the original agreement, each such investor received Common Units based on the fraction, the numerator of which was the Common Preference Amount due such Common Investor and the denominator of which was 1.17.
(b) Issuance of Convertible Bridge Notes
In 2017, the Company completed its offering of Convertible Bridge Note aggregating $19,965,091. The terms and conditions associated with these notes were consistent with the Convertible Bridge Notes issued during 2016 (see Note 12)
F-23
Table of Contents
ELECTROCORE, LLC, SUBSIDIARIES AND AFFILIATE
Notes to Consolidated Financial Statements—(Continued)
December 31, 2016
(c) Conversion of Bridge Notes
In connection with the initial closing under the Series B Preferred Unit Purchase Agreement entered into in August 2017 (see Note 17(a)), all outstanding Bridge Notes (aggregating $25,586,220), together with all related accrued and unpaid interest aggregating $1,132,690, were automatically converted into Series B Preferred Units, at $0.70 per Unit.
(d) Closing of Series B Preferred Units
In 2017, the Company completed closings of Series B Preferred Units aggregating $73,630,210 (inclusive of amounts mentioned above related to Bridge Notes and related accrued and unpaid interest). In connection with such closing, the Company also issued warrants for the purchase of 35,452,084 of the Company’s Common Units at an exercise price of $1.25 per Unit.
F-24
Table of Contents
Through and including , 2018 (the 25th day after the date of this prospectus), all dealers effecting transactions in these securities, whether or not participating in this offering, may be required to deliver a prospectus. This delivery requirement is in addition to a dealer’s obligation to deliver a prospectus when acting as an underwriter and with respect to an unsold allotment or subscription.
Shares

Common Stock
PROSPECTUS
Piper Jaffray
Evercore ISI
JMP Securities
, 2018
Table of Contents
PART II
INFORMATION NOT REQUIRED IN PROSPECTUS
| Item 13. | Other Expenses of Issuance and Distribution. |
The following table sets forth the costs and expenses, other than the underwriting discounts and commissions, payable by the registrant in connection with the sale of common stock being registered. All amounts are estimates except for the Securities and Exchange Commission, or SEC, registration fee, the FINRA filing fee and The Nasdaq Global Select Market listing fee.
| Item |
Amount to be paid |
|||
| SEC registration fee |
$ | * | ||
| FINRA filing fee |
* | |||
| The Nasdaq Global Select Market Listing fee |
* | |||
| Printing and engraving expenses |
* | |||
| Legal fees and expenses |
* | |||
| Accounting fees and expenses |
* | |||
| Blue Sky, qualification fees and expenses |
* | |||
| Transfer Agent fees and expenses |
* | |||
| Miscellaneous expenses |
* | |||
|
|
|
|||
| Total |
$ | * | ||
|
|
|
|||
| * | To be provided by amendment |
| Item 14. | Indemnification of Directors and Officers. |
Prior to the closing of this offering, Electrocore, LLC intends to convert into a Delaware corporation pursuant to a statutory conversion and change its name to electroCore, Inc. As permitted by Section 102 of the Delaware General Corporation Law, our certificate of incorporation and bylaws to be effective upon the corporate conversion will contain provisions that limit or eliminate the personal liability of our directors for a breach of their fiduciary duty of care as a director. The duty of care generally requires that, when acting on behalf of the corporation, directors exercise an informed business judgment based on all material information reasonably available to them. Consequently, a director will not be personally liable to us or our stockholders for monetary damages for breach of fiduciary duty as a director, except for liability for:
| • | any breach of the director’s duty of loyalty to us or our stockholders; |
| • | any act or omission not in good faith or that involves intentional misconduct or a knowing violation of law; |
| • | any act related to unlawful stock repurchases, redemptions or other distributions or payment of dividends; or |
| • | any transaction from which the director derived an improper personal benefit. |
These limitations of liability do not affect the availability of equitable remedies such as injunctive relief or rescission. Our certificate of incorporation will also authorize us to indemnify our officers, directors and other agents to the fullest extent permitted under Delaware law.
As permitted by Section 145 of the Delaware General Corporation Law, our bylaws will provide that:
| • | we may indemnify our directors, officers, and employees to the fullest extent permitted by the Delaware General Corporation Law, subject to limited exceptions; |
II-1
Table of Contents
| • | we may advance expenses to our directors, officers and employees in connection with a legal proceeding to the fullest extent permitted by the Delaware General Corporation Law, subject to limited exceptions; and |
| • | the rights provided in our bylaws are not exclusive. |
Our certificate of incorporation to be in effect upon the corporate conversion, attached as Exhibit 3.1 hereto, and our bylaws to be in effect upon the corporate conversion, attached as Exhibit 3.2 hereto, provide for the indemnification provisions described above and elsewhere herein. We intend to enter into separate indemnification agreements with our directors and officers which may be broader than the specific indemnification provisions contained in the Delaware General Corporation Law. These indemnification agreements will generally require us, among other things, to indemnify our officers and directors against liabilities that may arise by reason of their status or service as directors or officers, other than liabilities arising from willful misconduct. These indemnification agreements will also generally require us to advance any expenses incurred by the directors or officers as a result of any proceeding against them as to which they could be indemnified. In addition, we have purchased a policy of directors’ and officers’ liability insurance that insures our directors and officers against the cost of defense, settlement or payment of a judgment in some circumstances. These indemnification provisions and the indemnification agreements may be sufficiently broad to permit indemnification of our officers and directors for liabilities, including reimbursement of expenses incurred, arising under the Securities Act of 1933, as amended, or the Securities Act.
The form of Underwriting Agreement, attached as Exhibit 1.1 hereto, provides for indemnification by the underwriters of us and our officers who sign this Registration Statement and directors for specified liabilities, including matters arising under the Securities Act.
| Item 15. | Recent Sales of Unregistered Securities. |
The following sets forth information regarding all unregistered securities sold by us since January 1, 2015 through the date of the prospectus that forms a part of this registration statement.
| • | From January 2015 through March 2016, we issued Series A Preferred Units for aggregate consideration of $13.8 million. In connection with such transactions, we issued 16,193,018 million Series A Preferred Units. |
| • | In November 2015, we issued 2,266,741 Series A Preferred Units to existing investors at a purchase price of approximately $0.74 per unit, for aggregate consideration of approximately $1.7 million, in connection with the exercise of warrants to purchase our Series A Preferred Units. |
| • | In December 2015, we issued 66,177 warrants to purchase Series A Preferred Units to Core Ventures II, LLC, in connection a Loan and Security Agreement, pursuant to which we borrowed $1.25 million. |
| • | In December 2015, we issued 66,177 warrants to purchase Series A Preferred Units to Pacific Western Bank, in connection with a Loan and Security Agreement, pursuant to which we borrowed $1.25 million. |
| • | In March 2016, we issued 2,266,741 Series A Preferred Units at a purchase price of approximately $0.74 per unit, for aggregate consideration of approximately $1.67 million, in connection with the exercise of warrants to purchase Series A Preferred Units. |
| • | From June 2016 through August 2016, we issued convertible promissory notes of $1.5 million. We issued 1,795,407 Series A Preferred Units when such notes converted in September 2016. |
II-2
Table of Contents
| • | From September 2016 through June 2017, we issued Series B convertible promissory notes for aggregate consideration of $25.6 million. In connection with such transactions, we issued an aggregate of 41.9 million Common Units and warrants to purchase 7.31 million Series B Preferred Units, including to existing investors, investors affiliated with members of our board of directors, and our placement agents. |
| • | In July 2017, we issued 18.34 million Common Units to existing investors who committed to invest $9.17 million into our Series B financing. |
| • | From August 2017 through November 2017, we issued Series B Preferred Units for aggregate consideration of $73.6 million. In connection with such transactions, we issued 105.2 million Series B Preferred Units, and warrants to purchase 11.78 million Common Units, including to existing investors, those affiliated with members of our board of directors and our placement agents. |
| • | Since January 1, 2015, we have granted, net of forfeitures, 52.0 million Profits Interests to employees, consultants and certain members of our board of directors. |
We claimed exemption from registration under the Securities Act for the sales and issuances of securities in the transactions described above under Section 4(a)(2) of the Securities Act and/or Regulation D promulgated thereunder, in that such sales and issuances did not involve a public offering, or under Rule 701 promulgated under the Securities Act, in that they were offered and sold either pursuant to written compensatory plans or pursuant to a written contract relating to compensation, as provided by Rule 701. All of the purchasers of unregistered securities for which we relied on Section 4(a)(2) and/or Regulation D represented that they were accredited investors as defined under the Securities Act.
| Item 16. | Exhibits and Financial Statement Schedules. |
(a) Exhibits.
| Exhibit No. |
||||
| 1 | .1* | Form of Underwriting Agreement | ||
| 3 | .1* | Form of Certificate of Incorporation of electroCore, Inc. (to be effective upon completion of the Registrant’s conversion from a limited liability company to a corporation) | ||
| 3 | .2* | Form of Bylaws of electroCore, Inc. (to be effective upon completion of the Registrant’s conversion from a limited liability company to a corporation) | ||
| 4 | .1* | Specimen Stock Certificate evidencing the shares of common stock | ||
| 5 | .1* | Opinion of Dentons US LLP | ||
| 10 | .1* | Second Amended and Restated Limited Liability Company Agreement, dated as of August 18, 2017, by and among ElectroCore, LLC and the members party thereto | ||
| 10 | .2* | Third Amended and Restated Limited Liability Company Agreement, dated as of November 21, 2017, by and among ElectroCore, LLC and the members party thereto | ||
| 10 | .3* | Investors’ Rights Agreement, dated as of March 28, 2013, by and among ElectroCore, LLC and the investors party thereto | ||
| 10 | .4* | Amended and Restated Investors’ Rights Agreement, dated as of August 18, 2017, by and among Electrocore, LLC and the investors party thereto | ||
| 10 | .5*† | Form of ElectroCore, LLC Profits Interest Unit Forfeiture Agreement | ||
| 10 | .6*† | electroCore, Inc. 2018 Omnibus Equity Incentive Plan | ||
II-3
Table of Contents
| Exhibit No. |
||||
| 10 | .7*† | Form of Incentive Stock Option Agreement for electroCore, Inc. 2018 Omnibus Equity Incentive Plan | ||
| 10 | .8*† | Form of Restricted Stock Award Agreement for electroCore, Inc. 2018 Omnibus Equity Incentive Plan | ||
| 10 | .9*† | Form of Indemnification Agreement between the Registrant and each of its executive officers and directors | ||
| 10 | .10*† | Employment Offer Letter, dated as of July 18, 2016, by and between ElectroCore, LLC and Francis R. Amato | ||
| 10 | .11*† | Employment Offer Letter, dated as of July 18, 2017, by and between ElectroCore, LLC and Joseph P. Errico | ||
| 10 | .12*† | Employment Offer Letter, dated as of May 1, 2017, by and between ElectroCore, LLC and Peter S. Staats | ||
| 10 | .13*† | Employment Offer Letter, dated as of July 25, 2016, by and between ElectroCore, LLC and Glenn S. Vraniak | ||
| 10 | .14* | Office Lease between 150 Allen Road, LLC and Electrocore, LLC | ||
| 21 | .1* | List of subsidiaries of Electrocore, LLC | ||
| 23 | .1* | Consent of Dentons US LLP (included as part of Exhibit 5.1) | ||
| 23 | .2* | Consent of KPMG LLP, independent registered public accounting firm | ||
| 24 | .1 | Powers of Attorney (included on signature pages) | ||
| * | To be filed by amendment. |
| † | Indicates management agreement. |
| ‡ | Confidential treatment to be requested with respect to certain portions of this exhibit. Omitted portions to be filed separately with the Securities and Exchange Commission. |
(b) Financial Statement Schedules. Schedules not listed above have been omitted because the information required to be set forth therein is not applicable or is shown in the financial statements or notes thereto.
| Item 17. | Undertakings. |
Insofar as indemnification for liabilities arising under the Securities Act may be permitted to directors, officers and controlling persons of the Registrant pursuant to the foregoing provisions, or otherwise, the Registrant has been advised that in the opinion of the SEC such indemnification is against public policy as expressed in the Securities Act, and is, therefore, unenforceable. In the event that a claim for indemnification against such liabilities (other than the payment by the Registrant of expenses incurred or paid by a director, officer, or controlling person of the Registrant in the successful defense of any action, suit or proceeding) is asserted by such director, officer or controlling person in connection with the securities being registered, the Registrant will, unless in the opinion of its counsel the matter has been settled by controlling precedent, submit to a court of appropriate jurisdiction the question of whether such indemnification by it is against public policy as expressed in the Securities Act and will be governed by the final adjudication of such issue.
II-4
Table of Contents
The undersigned Registrant hereby undertakes that:
| 1. | For purposes of determining any liability under the Securities Act, the information omitted from the form of prospectus filed as part of this Registration Statement in reliance upon Rule 430A and contained in a form of prospectus filed by the Registrant pursuant to Rule 424(b)(1) or (4) or 497(h) under the Securities Act shall be deemed to be part of this Registration Statement as of the time it was declared effective. |
| 2. | For the purpose of determining any liability under the Securities Act, each post-effective amendment that contains a form of prospectus shall be deemed to be a new registration statement relating to the securities offered therein, and the offering of such securities at that time shall be deemed to be the initial bona fide offering thereof. |
The undersigned Registrant hereby undertakes to provide to the underwriters at the closing specified in the underwriting agreement certificates in such denominations and registered in such names as required by the underwriters to permit prompt delivery to each purchaser.
II-5
Table of Contents
SIGNATURES
Pursuant to the requirements of the Securities Act of 1933, as amended, the Registrant has duly caused this Registration Statement to be signed on its behalf by the undersigned, thereunto duly authorized, in the City of Basking Ridge, State of New Jersey, on this day of 2018.
| ELECTROCORE, LLC | ||
| By |
||
| Francis R. Amato | ||
| Chief Executive Officer | ||
POWER OF ATTORNEY
KNOW ALL PERSONS BY THESE PRESENTS, that each person whose signature appears below hereby constitutes and appoints Francis R. Amato and Glenn S. Vraniak, and each of them, as his true and lawful attorneys-in-fact, proxies and agents, each with full power of substitution, for him in any and all capacities, to sign any and all amendments to this registration statement (including post-effective amendments or any abbreviated registration statement and any amendments thereto filed pursuant to Rule 462(b) increasing the number of securities for which registration is sought), and to file the same, with all exhibits thereto and other documents in connection therewith, with the Securities and Exchange Commission, granting unto said attorneys-in-fact, proxies and agents full power and authority to do and perform each and every act and thing requisite and necessary to be done in connection therewith, as fully for all intents and purposes as he might or could do in person, hereby ratifying and confirming all that said attorneys-in-fact, proxies and agents, or their or his substitute or substitutes, may lawfully do or cause to be done by virtue hereof.
Pursuant to the requirements of the Securities Act, this Registration Statement has been signed by the following persons in the capacities and on the dates indicated.
| Signature |
Title |
Date | ||
|
Francis R. Amato |
Chief Executive Officer and Director (Principal Executive Officer) |
, 2018 | ||
|
Glenn S. Vraniak |
Chief Financial Officer |
, 2018 | ||
|
Joseph P. Errico |
Chairman of the Board |
, 2018 | ||
|
Nicholas Colucci |
Director |
, 2018 | ||
|
Dr. Thomas J. Errico |
Director |
, 2018 | ||
|
Trevor J. Moody |
Director |
, 2018 | ||
II-6
Table of Contents
| Signature |
Title |
Date | ||
|
Dr. David M. Rubin |
Director |
, 2018 | ||
|
James L.L. Tullis |
Director |
, 2018 | ||
II-7
Table of Contents
EXHIBIT INDEX
| Exhibit No. |
||||
| 1 | .1* | Form of Underwriting Agreement | ||
| 3 | .1* | Form of Certificate of Incorporation of electroCore, Inc. (to be effective upon completion of the Registrant’s conversion from a limited liability company to a corporation) | ||
| 3 | .2* | Form of Bylaws of electroCore, Inc. (to be effective upon completion of the Registrant’s conversion from a limited liability company to a corporation) | ||
| 4 | .1* | Specimen Stock Certificate evidencing the shares of common stock | ||
| 5 | .1* | Opinion of Dentons US LLP | ||
| 10 | .1* | Second Amended and Restated Limited Liability Company Agreement, dated as of August 18, 2017, by and among ElectroCore, LLC and the members party thereto | ||
| 10 | .2* | Third Amended and Restated Limited Liability Company Agreement, dated as of November 21, 2017, by and among ElectroCore, LLC and the members party thereto | ||
| 10 | .3* | Investors’ Rights Agreement, dated as of March 28, 2013, by and among ElectroCore, LLC and the investors party thereto | ||
| 10 | .4* | Amended and Restated Investors’ Rights Agreement, dated as of August 18, 2017, by and among Electrocore, LLC and the investors party thereto | ||
| 10 | .5*† | Form of ElectroCore, LLC Profits Interest Unit Forfeiture Agreement | ||
| 10 | .6*† | electroCore, Inc. 2018 Omnibus Equity Incentive Plan | ||
| 10 | .7*† | Form of Incentive Stock Option Agreement for electroCore, Inc. 2018 Omnibus Equity Incentive Plan | ||
| 10 | .8*† | Form of Restricted Stock Award Agreement for electroCore, Inc. 2018 Omnibus Equity Incentive Plan | ||
| 10 | .9*† | Form of Indemnification Agreement between the Registrant and each of its executive officers and directors | ||
| 10 | .10*† | Employment Offer Letter, dated as of July 18, 2016, by and between ElectroCore, LLC and Francis R. Amato | ||
| 10 | .11*† | Employment Offer Letter, dated as of July 18, 2017, by and between ElectroCore, LLC and Joseph P. Errico | ||
| 10 | .12*† | Employment Offer Letter, dated as of May 1, 2017, by and between ElectroCore, LLC and Peter S. Staats | ||
| 10 | .13*† | Employment Offer Letter, dated as of July 25, 2016, by and between ElectroCore, LLC and Glenn S. Vraniak | ||
| 10 | .14* | Office Lease between 150 Allen Road, LLC and Electrocore, LLC | ||
| 21 | .1* | List of subsidiaries of Electrocore, LLC | ||
| 23 | .1* | Consent of Dentons US LLP (included as part of Exhibit 5.1) | ||
| 23 | .2* | Consent of KPMG LLP, independent registered public accounting firm | ||
| 24 | .1 | Powers of Attorney (included on signature pages) | ||
| * | To be filed by amendment. |
| † | Indicates management agreement. |
| ‡ | Confidential treatment to be requested with respect to certain portions of this exhibit. Omitted portions to be filed separately with the Securities and Exchange Commission. |
II-8